| DRUGS INDEX | MANUFACTURERS INDEX | ANATOMY | GEOGRAPHY | USA STATISTICS | CHINA STATISTICS | RELIGION | JOBS |
 |
||
Elitek (Sanofi-Aventis) | ||
|
- Drugs index - Manufacturers - Feedback 
|
BOXED WARNINGS
DESCRIPTIONELITEK (rasburicase) is a recombinant urate-oxidase enzyme produced by a genetically modified Saccharomyces cerevisiae strain. The cDNA coding for rasburicase was cloned from a strain of Aspergillus flavus . Rasburicase is a tetrameric protein with identical subunits of a molecular mass of about 34 kDa. The molecular formula of the monomer is C 1523 H 2383 N 417 O 462 S 7 . The monomer, made up of a single 301 amino acid polypeptide chain, has no intra- or inter-disulfide bridges and is N-terminal acetylated. The drug product is a sterile, white to off-white, lyophilized powder intended for intravenous administration following reconstitution. ELITEK is supplied in 3-mL colorless, glass vials containing 1.5 mg rasburicase, 10.6 mg mannitol, 15.9 mg L-alanine, and between 12.6 and 14.3 mg of dibasic sodium phosphate. The diluent solution for reconstitution, supplied in a 2 mL clear, glass ampule, is composed of 1.0 mL sterile Water for Injection, USP, and 1.0 mg Poloxamer 188. The product reconstituted with diluent is a clear, colorless solution.
CLINICAL PHARMACOLOGYIn humans, uric acid is the final step in the catabolic pathway of purines. Rasburicase catalyzes enzymatic oxidation of uric acid into an inactive and soluble metabolite (allantoin). Rasburicase is only active at the end of the purine catabolic pathway. Pharmacokinetics of rasburicase were evaluated in two studies that enrolled patients with lymphoid leukemia (B and T cell), non-Hodgkin's lymphoma (including Burkitt's lymphoma) or acute myelogenous leukemia. ELITEK exposure, as measured by AUC 0-24 hr and C max , tended to increase linearly with doses over a limited dose range (0.15 to 0.20 mg/kg). The overall elimination half-life was 18 hours. No accumulation of rasburicase was observed between days 1 and 5 of dosing. ELITEK mean volume of distribution was 110 to 127 mL/kg in pediatric patients. There are insufficient data to characterize pharmacokinetics in adult patients.
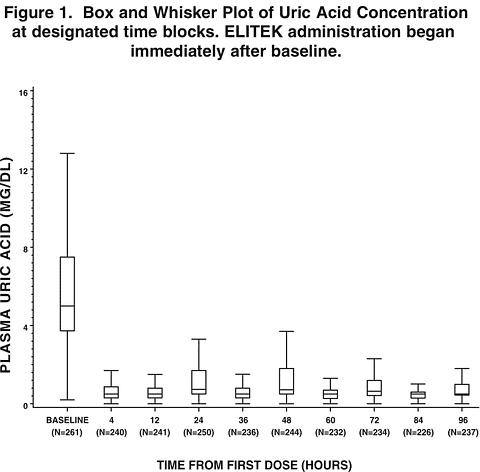
CLINICAL STUDIESELITEK was administered in three studies to 265 patients with acute leukemia or non-Hodgkin's lymphoma. The clinical studies were largely limited to pediatric patients (246 of 265). ELITEK was administered as a 30-minute infusion once (n=251) or twice (n=14) daily at a dose of 0.15 or 0.20 mg/kg/dose (total daily dose 0.20-0.40 mg/kg/day). ELITEK was administered prior to and concurrent with anti-tumor therapy, which consisted of either systemic chemotherapy (n=196) or steroids (n=69). Study 1Study 1 was a randomized, open-label, controlled study conducted at six institutions, in which 52 pediatric patients were randomized to receive either ELITEK (n=27) or allopurinol (n=25). 1 The dose of allopurinol varied according to local institutional practice. ELITEK was administered as an intravenous infusion over 30 minutes once (n=26) or twice (n=1) daily at a dose of 0.20 mg/kg/dose (total daily dose 0.20-0.40 mg/kg/day). Initiation of dosing was permitted at any time between 4 to 48 hours before the start of anti-tumor therapy and could be continued for 5 to 7 days after initiation of anti-tumor therapy. Patients were stratified at randomization on the basis of underlying malignant disease (leukemia or lymphoma) and baseline serum or plasma uric acid levels (<8.0 mg/dL and >/=8.0 mg/dL). The primary study objective was to demonstrate a greater reduction in uric acid concentration over 96 hours (AUC 0-96 hr ) in the ELITEK group as compared to the allopurinol group. Uric acid AUC 0-96 hr was defined as the area under the curve for plasma uric acid levels (mg·hr/dL), measured from the last value prior to the first dose of ELITEK until 96 hours after that first dose. Plasma uric acid levels were used for all uric acid AUC 0-96 hr calculations (see PRECAUTIONS , Laboratory Test Interactions ). The demographics of the two study arms (ELITEK vs. allopurinol) were as follows: age <13 years (82% vs. 76%), males (59% vs. 72%), Caucasian (59% vs. 72%), ECOG performance status 0 (89% vs. 84%), and leukemia (74% vs. 76%). The median interval, in hours, between initiation of ELITEK and of anti-tumor treatment was 20 hours, with a range of 70 hours before to 10 hours after the initiation of anti-tumor treatment (n=24, data not reported for 3 patients). The uric acid AUC 0-96 hr was significantly lower in the ELITEK group (128 ± s.e. 14 mg·hr/dL) as compared to the allopurinol group (328 ± s.e. 26 mg·hr/dL). All but one patient in the ELITEK arm had reduction and maintenance of uric acid levels to within or below the normal range during the treatment. The incidence of renal dysfunction was similar in the two study arms; one patient in the allopurinol arm developed acute renal failure. Study 2Study 2 was a multi-institutional, single-arm study conducted in 89 pediatric and 18 adult patients with hematologic malignancies. Patients received ELITEK at a dose of 0.15 mg/kg/day. The primary efficacy objective was determination of the proportion of patients with maintained plasma uric acid concentration at 48 hours where maintenance of uric acid concentration was defined as: 1) achievement of uric acid concentration </=6.5 mg/dL (patients <13 years) or </=7.5 mg/dL (patients >/=13 years) within a designated time point (48 hours) from initiation of ELITEK and maintained until 24 hours after the last administration of study drug; and 2) control of uric acid level without the need for allopurinol or other agents. The study population demographics were: age <13 years (76%), males (61%), Caucasian (91%), ECOG performance status = 0 (92%), and leukemia (89%). The proportion of patients with maintenance of uric acid concentration at 48 hours in Study 2 was 99% (106/107). Study 3Study 3 was a multi-institutional, single-arm study conducted in 130 pediatric patients and 1 adult patient with hematologic malignancies. 2 Patients received ELITEK at either a dose of 0.15 mg/kg/day (n=12) or 0.20 mg/kg/day (n=119). The primary efficacy objective was determination of the proportion of patients with maintained plasma uric acid concentration at 48 hours as defined for Study 2 above. The study population demographics were: age <13 years (76%), Caucasian (83%), males (67%), ECOG = 0 (67%), and leukemia (88%). The proportion of patients with maintenance of uric acid concentration at 48 hours in Study 3 was 92% in the 0.15 mg/kg group (n=12) and 95% in the 0.20 mg/kg group (n=119). Pooled AnalysesDosing For the pooled data set of the 3 clinical studies (n=265), total daily dosing for ELITEK ranged from 0.15 to 0.40 mg/kg/day with the majority receiving 0.20 mg/kg/day. The maximum daily doses received were 0.15 mg/kg/day in 116 patients, 0.20 mg/kg/day in 135 patients, 0.30 mg/kg/day (divided doses) in 3 patients, and 0.40 mg/kg/day (di-vided doses) in 11 patients. The safety and effectiveness of twice-daily dosing with ELITEK have not been established due to insufficient data (see DOSAGE AND ADMINISTRATION ). Reduction of Uric Acid Levels Data from the 3 studies (n=265) were pooled and analyzed according to the plasma uric acid levels over time. The pre-treatment plasma uric acid concentration was >/=8 mg/dL in 61 patients and was <8 mg/dL in 200 patients. The median uric acid concentration at baseline, at 4 hours following the first dose of ELITEK, and the per patient fall in plasma uric acid concentration from baseline to 4 hours were calculated in those patients with both pre-treatment and 4-hour post-treatment values. Among patients with pre-treatment uric acid >/=8.0 mg/dL [baseline median 10.6 mg/dL (range 8.1-36.4)], the median per-patient change in plasma uric acid concentration by 4 hours after the first dose was a decrease of 9.1 mg/dL (0.3-19.3 mg/dL). Among the patients with a pre-treatment plasma uric acid level < 8 mg/dL [baseline median 4.6 mg/dL (range 0.2-7.9 mg/dL)], the median per-patient change in plasma uric acid concentration by 4 hours after the first dose was a decrease of 4.1 mg/dL (0.1-7.6 mg/dL).
Figure 1 is a box and whisker plot of plasma uric acid levels inclusive of 261 of the 265 ELITEK treated patients from Studies 1, 2, and 3. Of the 261 evaluable patients, plasma uric acid concentration was maintained (see CLINICAL STUDIES , Study 2 , for the definition of uric acid concentration maintenance) by 4 hours for 92% of patients (240/261), by 24 hours for 93% of patients (245/261), by 48 hours for 97% of patients (254/261), by 72 hours for 99% of patients (260/261), and by 96 hours for 100% of patients (261/261). Of the subset of 61 patients whose plasma uric acid level was elevated at baseline (>/=8 mg/dL), plasma uric acid concentration was maintained by 4 hours for 72% of patients (44/61), by 24 hours for 80% of patients (49/61), by 48 hours for 92% of patients (56/61), by 72 hours for 98% of patients (60/61), and by 96 hours for 100% (61/61).
INDICATIONS AND USAGEELITEK (rasburicase) is indicated for the initial management of plasma uric acid levels in pediatric patients with leukemia, lymphoma, and solid tumor malignancies who are receiving anti-cancer therapy expected to result in tumor lysis and subsequent elevation of plasma uric acid.
CONTRAINDICATIONSELITEK is contraindicated in individuals deficient in glucose-6-phosphate dehydrogenase (G6PD) (see BOXED WARNINGS , Hemolysis and WARNINGS , Hemolysis ). ELITEK is contraindicated in patients with a known history of anaphylaxis or hypersensitivity reactions, hemolytic reactions or methemoglobinemia reactions to ELITEK or any of the excipients (see BOXED WARNINGS and WARNINGS ).
WARNINGSAnaphylaxisThe safety and efficacy of ELITEK have been established only for a single course of treatment [once daily for 5 days (see DOSAGE AND ADMINISTRATION )]. ELITEK may cause severe allergic reactions including anaphylaxis. This can occur at any time during treatment including the first dose. Signs and symptoms of these reactions include bronchospasm, chest pain and tightness, dyspnea, hypoxia, hypotension, shock, and/or urticaria. ELITEK administration should be immediately and permanently discontinued in any patient developing clinical evidence of a serious hypersensitivity reaction (see BOXED WARNINGS , Anaphylaxis and ADVERSE REACTIONS , Immunogenicity ). HemolysisELITEK is contraindicated in patients with G6PD deficiency because hydrogen peroxide is one of the major by-products of the conversion of uric acid to allantoin. In clinical studies, two patients developed severe hemolytic reactions [National Cancer Institute Common Toxicity Criteria 3 (NCI CTC) grade 3 and 4] within 2-4 days of the start of ELITEK. G6PD deficiency was subsequently identified in one of these patients. ELITEK administration should be immediately and permanently discontinued in any patient developing hemolysis, and appropriate patient monitoring and support measures initiated (e.g., transfusion support). It is recommended that patients at higher risk for G6PD deficiency (e.g., patients of African or Mediterranean ancestry) be screened prior to starting ELITEK therapy (see BOXED WARNINGS , Hemolysis and CONTRAINDICATIONS ). MethemoglobinemiaIn clinical studies, methemoglobinemia has been reported in 2 patients receiving ELITEK. Both patients developed serious hypoxemia requiring intervention with the appropriate medical support measures. It is not known whether patients with deficiency of cytochrome b5 reductase (formerly known as methemoglobin reductase) or of other enzymes with antioxidant activity are at increased risk for methemoglobinemia or hemolytic anemia. ELITEK administration should be immediately and permanently discontinued in any patient identified as having developed methemoglobinemia, and appropriate monitoring and support mea-sures (e.g., transfusion support, methylene-blue ad-ministration) implemented (see BOXED WARNINGS , Methemoglobinemia ).
PRECAUTIONSGeneralPatients on ELITEK should receive intravenous hydration according to standard medical practice for the management of plasma uric acid in patients at risk for tumor lysis syndrome. Drug InteractionsNo studies of interactions with other drugs have been conducted in humans. Rasburicase does not metabolize allopurinol, cytarabine, methylprednisolone, methotrexate, 6-mercaptopurine, thioguanine, etoposide, daunorubicin, cyclophosphamide or vincristine in vitro . No metabolic-based drug interactions are therefore anticipated with these agents in patients. In preclinical in vivo studies, rasburicase did not affect the activity of isoenzymes CYP1A, CYP2A, CYP2B, CYP2C, CYP2E, and CYP3A, suggesting no induction nor inhibition potential. Clinically relevant P450-mediated drug-drug interactions are therefore not anticipated in patients treated with the recommended ELITEK dose and dosing schedule. Laboratory Test InteractionsAt room temperature, ELITEK causes enzymatic degradation of the uric acid in blood/plasma/serum samples potentially resulting in spuriously low plasma uric acid assay readings. The following special sample handling procedure must be followed to avoid ex vivo uric acid degradation. Uric acid must be analyzed in plasma. Blood must be collected into prechilled tubes containing heparin anticoagulant. Samples must be immediately immersed in an ice water bath . Plasma samples must be prepared by centrifugation in a pre-cooled centrifuge (4°C). Finally, the plasma must be maintained in an ice water bath and analyzed for uric acid within four hours of collection (see BOXED WARNINGS , Interference with Uric Acid Measurement ). Carcinogenesis, Mutagenesis, Impairment of FertilityLong-term studies in animals to evaluate carcinogenic potential have not been performed. ELITEK was non-genotoxic in the Ames, unscheduled DNA synthesis, chromosome analysis, mouse lymphoma, and micronucleus tests. ELITEK did not affect reproductive performance or fertility in male or female rats at doses 8-fold higher than the human dose when corrected for differences in body surface area. Pregnancy Category CAnimal reproduction studies have not been conducted with ELITEK. It is also not known whether ELITEK can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. ELITEK should be given to a pregnant woman only if clearly needed. Nursing MothersIt is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants, a decision should be made whether to discontinue nursing or to discontinue ELITEK, taking into account the importance of the drug to the mother. Pediatric UseThe efficacy and safety of ELITEK was studied in 246 pediatric patients ranging in age from 1 month to 17 years. There were an insufficient number of patients in the 0-6 months age group (n=7) to determine whether they respond differently from older children. These patients were pooled into the <2 years of age group (n=24). Children <2 years of age had a higher mean uric acid AUC 0-96 hr than those age 2-17 years (150 ± s.e. 16 mg·hr/dL vs. 108 ± s.e. 4 mg·hr/dL, respectively). In addition, the data suggest that children <2 years of age had a lower rate of success at achieving maintenance uric acid concentration by 48 hours [83% (95% CI of 62 to 95) vs. 93% (95% CI of 89 to 95), respectively]. Children <2 years old also experienced more toxicity. The following adverse events were observed more frequently in children less than 2 years of age compared to those age 2-17 years respectively: vomiting (75% vs. 55%), diarrhea (63% vs. 20%), fever (50% vs. 38%), and rash (38% vs. 10%). Geriatric UseFive of the 19 adults among the 265 patients enrolled in clinical studies of ELITEK, were age 65 or greater. Therefore, there are insufficient data to determine whether geriatric subjects, or adults in general, respond differently from pediatric subjects.
ADVERSE REACTIONSBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The adverse reaction information from clinical trials does, however, provide a basis for identifying the adverse events that appear to be related to drug use and for approximating rates. The data described below reflect exposure to ELITEK in 703 patients [63% male, 37% female; median age 10 years (range 10 days to 88 years); 73% Caucasian, 9% African, 4% Asian, 14% other/unknown]. ELITEK was studied for adverse reactions, regardless of severity, in 347 patients (265 pediatric and 82 adults) enrolled in one active-controlled trial (Study 1), two uncontrolled trials (Studies 2 and 3), and one uncontrolled safety trial (n=82). Additionally, an expanded access experience enrolled 356 patients, for whom reliably collected data were limited to serious adverse reactions. Among the 703 patients for whom serious adverse reactions were assessed, the most serious adverse reactions caused by ELITEK were allergic reactions including anaphylaxis (<1%), rash (1%), hemolysis (<1%), and methemoglobinemia (<1%) (see BOXED WARNINGS and WARNINGS ). The commonly observed serious adverse reactions were fever (5%), neutropenia with fever (4%), respiratory distress (3%), sepsis (3%), neutropenia (2%), and mucositis (2%). The following additional serious adverse reactions were observed in </=1% of patients regardless of causality: acute renal failure, arrhythmia, cardiac failure, cardiac arrest, cellulitis, cerebrovascular disorder, chest pain, convulsions, cyanosis, diarrhea, dehydration, hot flushes, ileus, infection, intestinal obstruction, hemorrhage, myocardial infarction, paresthesia, pancytopenia, pneumonia, pulmonary edema, pulmonary hypertension, retinal hemorrhage, rigors, thrombosis, and thrombophlebitis. Among the 347 patients for whom all adverse reactions regardless of severity were assessed, the most frequently observed adverse reactions (incidence >/=10%) were vomiting (50%), fever (46%), nausea (27%), headache (26%), abdominal pain (20%), constipation (20%), diarrhea (20%), mucositis (15%), and rash (13%). In Study 1, an active control study, the following adverse events occurred more frequently in ELITEK-treated subjects than allopurinol-treated subjects: vomiting, fever, nausea, diarrhea, and headache. Although the incidence of rash was similar in the two arms, severe rash (NCI CTC 3 , Grade 3 or 4) was reported only in one ELITEK-treated patient. ImmunogenicityELITEK is immunogenic in healthy volunteers, and can elicit antibodies that inhibit the activity of rasburicase in vitro (see BOXED WARNINGS , Anaphylaxis and WARNINGS , Anaphylaxis ). In a study of 28 healthy volunteers, the incidence of antibody responses to either a single dose or to 5 daily doses was assessed. Binding antibodies to rasburicase were detected by ELISA in 17/28 (61%) volunteers and neutralizing antibodies were detected in 18/28 (64%) volunteers. Time to detection of antibodies ranged from 1 to 6 weeks after ELITEK exposure. In two subjects with extended follow-up, antibodies persisted for 333 and 494 days. The incidence of antibody responses in patients with hematologic malignancy has not been adequately assessed. In clinical trials of patients with hematologic malignancies, 24 of the 218 patients tested (11%) developed antibodies by day 28 following ELITEK administration. However, this is not a reliable estimate of the true incidence of antibody responses in patients with hematologic malignancies, because the data from the healthy volunteer study indicate that antibody may not be detectable until some time point beyond day 28. The incidence of antibody responses detected is highly dependent on the sensitivity and specificity of the assay, which have not been fully evaluated. Additionally, the observed incidence of antibody positivity in an assay may be influenced by several factors, including serum sampling, timing and methodology, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to ELITEK with the incidence of antibodies to other products may be misleading.
OVERDOSAGENo cases of overdosage with ELITEK have been reported. The maximum dose of ELITEK that has been administered as a single dose is 0.20 mg/kg; the maximum daily dose that has been administered is 0.40 mg/kg/day. According to the mechanism of action of ELITEK, an overdose will lead to low or undetectable plasma uric acid concentration, which has no known clinical consequences. Patients suspected of receiving an overdose should be monitored, and general supportive measures should be initiated as no specific antidote for ELITEK has been identified.
DOSAGE AND ADMINISTRATIONThe recommended dose and schedule of ELITEK is 0.15 or 0.20 mg/kg as a single daily dose for 5 days. Because the safety and effectiveness of other schedules have not been established, dosing beyond 5 days or administration of more than one course of ELITEK is not recommended. Chemotherapy should be initiated 4 to 24 hours after the first dose of ELITEK. DO NOT ADMINISTER AS A BOLUS INFUSION . ELITEK should be administered as an intravenous infusion over 30 minutes. Reconstitution ProcedureDetermine the number of vials of ELITEK needed to achieve the proper dosage, based on the individual patient's weight and the dose per kilogram. ELITEK must be reconstituted in the diluent provided. Add 1 mL of the provided reconstitution solution (diluent) to each vial of ELITEK and mix by swirling very gently. Do not shake or vortex . Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, and discarded if particulate matter is visible or if product is discolored. Further Dilution and AdministrationUsing aseptic technique and syringes of appropriate volume, remove the predetermined dose of ELITEK from the reconstituted vials and inject into an infusion bag containing the appropriate volume of 0.9% sterile sodium chloride, to achieve a final total volume of 50 mL. This final solution for injection is to be infused over 30 minutes. No filters should be used for the infusion. The reconstituted ELITEK contains no preservatives and must be administered within 24 hours of reconstitution. The reconstituted or diluted solution can be stored up to 24 hours at 2-8°C. Discard any unused product. ELITEK should be infused through a different line than that used for the infusion of other concomitant medications. If use of a separate line is not possible, the line should be flushed with at least 15 mL of saline solution prior to and after infusion with ELITEK.
HOW SUPPLIEDNDC 0024-5150-10: One carton containing 3 single-use vials each containing 1.5 mg of rasburicase and 3 ampules each containing 1.0 mL diluent. Storage and Handling The lyophilized drug product and the diluent for reconstitution should be stored at 2-8°C (36-46°F). Do not freeze. Protect from light.
REFERENCES
sanofi~synthelabo Manufactured and distributed by Sanofi-Synthelabo Inc. New York, NY 10016 U.S. License No. 1294 Printed in USA Revised March 2005 Copyright, Sanofi-Synthelabo Inc. 2002, 2005 5631 |
 - To bookmark this page (add it to your favorites), please click the image to the left.
- To bookmark this page (add it to your favorites), please click the image to the left.