










































ANNEX I
SUMMARY OF PRODUCT CHARACTERISTICS
1.
Lantus 100 units/ml solution for injection in a vial
2.
Each ml contains 100 units insulin glargine (equivalent to 3.64 mg).
Each vial contains 5 ml of solution for injection, equivalent to 500 units, or 10 ml of solution for
injection, equivalent to 1000 units.
Insulin glargine is produced by recombinant DNA technology in
Escherichia coli
.
For a full list of excipients, see section 6.1.
3.
Solution for injection.
Clear colourless solution.
4.
For the treatment of adults, adolescents and children of 6 years or above with diabetes mellitus, where
treatment with insulin is required.
Posology
Lantus contains insulin glargine, an insulin analogue, and has a prolonged duration of action.
Lantus should be administered once daily at any time but at the same time each day.
The Lantus dose regimen (dose and timing) should be individually adjusted. In patients with type 2
diabetes mellitus, Lantus can also be given together with orally active antidiabetic medicinal products.
The potency of this medicinal product is stated in units. These units are exclusive to Lantus and are
not the same as IU or the units used to express the potency of other insulin analogues. (see
section 5.1).
Elderly population (≥ 65 years old)
In the elderly, progressive deterioration of renal function may lead to a steady decrease in insulin
requirements.
Renal impairment
In patients with renal impairment, insulin requirements may be diminished due to reduced insulin
metabolism.
Hepatic impairment
In patients with hepatic impairment, insulin requirements may be diminished due to reduced capacity
for gluconeogenesis and reduced insulin metabolism.
2
Paediatric population
Safety and efficacy of Lantus have been established in adolescents and children of 6 years and above.
In children, efficacy and safety of Lantus have only been demonstrated when given in the evening.
Due to limited experience on the efficacy and safety of Lantus in children below the age of 6 years,
Lantus should only be used in this age group under careful medical supervision.
Transition from other insulins to Lantus
When changing from a treatment regimen with an intermediate or long-acting insulin to a regimen
with Lantus, a change of the dose of the basal insulin may be required and the concomitant
antidiabetic treatment may need to be adjusted (dose and timing of additional regular insulins or fast-
acting insulin analogues or the dose of oral antidiabetic medicinal products).
To reduce the risk of nocturnal and early morning hypoglycaemia, patients who are changing their
basal insulin regimen from a twice daily NPH insulin to a once daily regimen with Lantus should
reduce their daily dose of basal insulin by 20-30 % during the first weeks of treatment.
During the first weeks the reduction should, at least partially, be compensated by an increase in
mealtime insulin, after this period the regimen should be adjusted individually.
As with other insulin analogues, patients with high insulin doses because of antibodies to human
insulin may experience an improved insulin response with Lantus.
Close metabolic monitoring is recommended during the transition and in the initial weeks thereafter.
With improved metabolic control and resulting increase in insulin sensitivity a further adjustment in
dose regimen may become necessary. Dose adjustment may also be required, for example, if the
patient's weight or life-style changes, change of timing of insulin dose or other circumstances arise that
increase susceptibility to hypo-or hyperglycaemia (see section 4.4).
Method of administration
Lantus is administered subcutaneously.
Lantus should not be administered intravenously. The prolonged duration of action of Lantus is
dependent on its injection into subcutaneous tissue. Intravenous administration of the usual
subcutaneous dose could result in severe hypoglycaemia.
There are no clinically relevant differences in serum insulin or glucose levels after abdominal, deltoid
or thigh administration of Lantus. Injection sites must be rotated within a given injection area from one
injection to the next.
Lantus must not be mixed with any other insulin or diluted. Mixing or diluting can change its
time/action profile and mixing can cause precipitation.
For further details on handling, see section 6.6.
Hypersensitivity to the active substance or to any of the excipients.
3
Lantus is not the insulin of choice for the treatment of diabetic ketoacidosis. Instead, regular insulin
administered intravenously
is recommended in such cases.
In case of insufficient glucose control or a tendency to hyper- or hypoglycaemic episodes, the patient's
adherence to the prescribed treatment regimen, injection sites and proper injection technique and all
other relevant factors must be reviewed before dose adjustment is considered.
Transferring a patient to another type or brand of insulin should be done under strict medical
supervision. Changes in strength, brand (manufacturer), type (regular, NPH, lente, long-acting, etc.),
origin (animal, human, human insulin analogue) and/or method of manufacture may result in the need
for a change in dose.
Insulin administration may cause insulin antibodies to form. In rare cases, the presence of such insulin
antibodies may necessitate adjustment of the insulin dose in order to correct a tendency to hyper- or
hypoglycaemia. (see section 4.8)
Hypoglycaemia
The time of occurrence of hypoglycaemia depends on the action profile of the insulins used and may,
therefore, change when the treatment regimen is changed. Due to more sustained basal insulin supply
with Lantus, less nocturnal but more early morning hypoglycaemia can be expected.
Particular caution should be exercised, and intensified blood glucose monitoring is advisable in
patients in whom hypoglycaemic episodes might be of particular clinical relevance, such as in patients
with significant stenoses of the coronary arteries or of the blood vessels supplying the brain (risk of
cardiac or cerebral complications of hypoglycaemia) as well as in patients with proliferative
retinopathy, particularly if not treated with photocoagulation (risk of transient amaurosis following
hypoglycaemia).
Patients should be aware of circumstances where warning symptoms of hypoglycaemia are
diminished. The warning symptoms of hypoglycaemia may be changed, be less pronounced or be
absent in certain risk groups. These include patients:
-
in whom glycaemic control is markedly improved,
-
who are elderly,
-
after transfer from animal insulin to human insulin,
-
in whom an autonomic neuropathy is present,
-
with a long history of diabetes,
-
suffering from a psychiatric illness,
-
receiving concurrent treatment with certain other medicinal products (see section 4.5).
Such situations may result in severe hypoglycaemia (and possibly loss of consciousness) prior to the
patient's awareness of hypoglycaemia.
The prolonged effect of subcutaneous insulin glargine may delay recovery from hypoglycaemia.
If normal or decreased values for glycated haemoglobin are noted, the possibility of recurrent,
unrecognised (especially nocturnal) episodes of hypoglycaemia must be considered.
4
-
in whom hypoglycaemia develops gradually,
Adherence of the patient to
the dose and dietary regimen, correct insulin administration and awareness
of hypoglycaemia symptoms are essential to reduce the risk of hypoglycaemia. Factors increasing the
susceptibility to hypoglycaemia require particularly close monitoring and may necessitate dose
adjustment. These include:
-
change in the injection area,
-
improved insulin sensitivity (e.g., by removal of stress factors),
-
intercurrent illness (e.g. vomiting, diarrhoea),
-
inadequate food intake,
-
missed meals,
-
alcohol consumption,
-
certain uncompensated endocrine disorders, (e.g. in hypothyroidism and in anterior pituitary or
adrenocortical insufficiency),
-
concomitant treatment with certain other medicinal products.
Intercurrent illness
Intercurrent illness requires intensified metabolic monitoring. In many cases urine tests for ketones are
indicated, and often it is necessary to adjust the insulin dose. The insulin requirement is often
increased. Patients with type 1 diabetes must continue to consume at least a small amount of
carbohydrates on a regular basis, even if they are able to eat only little or no food, or are vomiting etc.
and they must never omit insulin entirely.
Medication errors
Medication errors have been reported in which other insulins, particularly short-acting insulins, have
been accidentally administered instead of insulin glargine. Insulin label must always be checked
before each injection to avoid medication errors between insulin glargine and other insulins.
Combination of Lantus with pioglitazone
Cases of cardiac failure have been reported when pioglitazone was used in combination with insulin,
especially in patients with risk factors for development of cardiac heart failure. This should be kept in
mind if treatment with the combination of pioglitazone and Lantus is considered. If the combination is
used, patients should be observed for signs and symptoms of heart failure, weight gain and oedema.
Pioglitazone should be discontinued if any deterioration in cardiac symptoms occurs.
A number of substances affect glucose metabolism and may require dose adjustment of insulin
glargine.
Substances that may enhance the blood-glucose-lowering effect and increase susceptibility to
hypoglycaemia include oral antidiabetic medicinal products, angiotensin converting enzyme (ACE)
inhibitors, disopyramide, fibrates, fluoxetine, monoamine oxidase (MAO) inhibitors, pentoxifylline,
propoxyphene, salicylates and sulfonamide antibiotics.
Substances that may reduce the blood-glucose-lowering effect include corticosteroids, danazol,
diazoxide, diuretics, glucagon, isoniazid, oestrogens and progestogens, phenothiazine derivatives,
somatropin, sympathomimetic medicinal products (e.g. epinephrine [adrenaline], salbutamol,
terbutaline), thyroid hormones, atypical antipsychotic medicinal products (e.g. clozapine and
olanzapine) and protease inhibitors.
Beta-blockers, clonidine, lithium salts or alcohol may either potentiate or weaken the blood-glucose-
lowering effect of insulin. Pentamidine may cause hypoglycaemia, which may sometimes be followed
by hyperglycaemia.
5
-
unaccustomed, increased or prolonged physical activity,
In addition, under the influence of sympatholytic medicinal products such as beta-blockers, clonidine,
guanethidine and reserpine, the signs of adrenergic counter-regulation may be reduced or absent.
Pregnancy
For insulin glargine no clinical data on exposed pregnancies from controlled clinical trials are
available.A moderate amount of data on pregnant women (between 300-1000 pregnancy outcomes)
exposed to marketed insulin glargine indicate no adverse effects of insulin glargine on pregnancy and
no malformative nor feto/neonatal toxicity of insulin glargine.
Animal data do not indicate reproductive toxicity.
The use of Lantus may be considered during pregnancy, if necessary.
It is essential for patients with pre-existing or gestational diabetes to maintain good metabolic control
throughout pregnancy. Insulin requirements may decrease during the first trimester and generally
increase during the second and third trimesters. Immediately after delivery, insulin requirements
decline rapidly (increased risk of hypoglycaemia). Careful monitoring of glucose control is essential.
Breastfeeding
It is unknown whether insulin glargine is excreted in human milk. No metabolic effects of ingested
insulin glargine on the breastfed newborn/infant are anticipated since insulin glargine as a peptide is
digested into aminoacids in the human gastrointestinal tract. Breastfeeding women may require
adjustments in insulin dose and diet.
Fertility
Animal studies do not indicate direct harmful effects with respect to fertility.
The patient's ability to concentrate and react may be impaired as a result of hypoglycaemia or
hyperglycaemia or, for example, as a result of visual impairment. This may constitute a risk in
situations where these abilities are of special importance (e.g. driving a car or operating machines).
Patients should be advised to take precautions to avoid hypoglycaemia whilst driving. This is
particularly important in those who have reduced or absent awareness of the warning symptoms of
hypoglycaemia or have frequent episodes of hypoglycaemia. It should be considered whether it is
advisable to drive or operate machines in these circumstances.
Hypoglycaemia, in general the most frequent adverse reaction of insulin therapy, may occur if the
insulin dose is too high in relation to the insulin requirement.
The following related adverse reactions from clinical investigations are listed below by system organ
class and in order of decreasing incidence (very common: ≥ 1/10; common: ≥ 1/100 to <1/10;
uncommon: ≥ 1/1,000 to < 1/100; rare: ≥ 1/10,000 to < 1/1,000; very rare: < 1/10,000).
6
Within each frequency grouping, adverse reactions are presented in order of decreasing seriousnes
s.
MedDRA
system organ
classes
Very common Common
Uncommon Rare
Veryrare
Immune system
disorders
Allergic
reactions
Metabolism and
nutrition
disorders
Hypoglycaemia
Nervous system
disorders
Dysgeusia
Eyes disorders
Visual
impairment
Retinopathy
Skin and
subcutaneous
tissue disorders
Lipohypertro-
phy
Lipoatrophy
Musculoskeletal
and connective
tissue disorders
Myalgia
General
disorders and
administration
site conditions
Injection site
reactions
Oedema
Metabolism and nutrition disorders
Severe hypoglycaemic attacks, especially if recurrent, may lead to neurological damage. Prolonged or
severe hypoglycaemic episodes may be life-threatening.
In many patients, the signs and symptoms of neuroglycopenia are preceded by signs of adrenergic
counter-regulation. Generally, the greater and more rapid the decline in blood glucose, the more
marked is the phenomenon of counter-regulation and its symptoms.
Immune system disorders
Immediate-type allergic reactions to insulin are rare. Such reactions to insulin (including insulin
glargine) or the excipients may, for example, be associated with generalised skin reactions, angio-
oedema, bronchospasm, hypotension and shock, and may be life-threatening.
Insulin administration may cause insulin antibodies to form. In clinical studies, antibodies that cross-
react with human insulin and insulin glargine were observed with the same frequency in both NPH-
insulin and insulin glargine treatment groups. In rare cases, the presence of such insulin antibodies
may necessitate adjustment of the insulin dose in order to correct a tendency to hyper- or
hypoglycaemia.
Eyes disorders
A marked change in glycaemic control may cause temporary visual impairment, due to temporary
alteration in the turgidity and refractive index of the lens.
Long-term improved glycaemic control decreases the risk of progression of diabetic retinopathy.
However, intensification of insulin therapy with abrupt improvement in glycaemic control may be
associated with temporary worsening of diabetic retinopathy. In patients with proliferative retinopathy,
7














particularly if not treated with photocoagulation, severe hypoglycaemic episodes may result in
transient amaurosis.
Skin and subcutaneous tissue disorders
As with any insulin therapy, lipodystrophy may occur at the injection site and delay local insulin
absorption. Continuous rotation of the injection site within the given injection area may help to reduce
or prevent these reactions.
General disorders and administration site conditions
Injection site reactions include redness, pain, itching, hives, swelling, or inflammation. Most minor
reactions to insulins at the injection site usually resolve in a few days to a few weeks.
Rarely, insulin may cause sodium retention and oedema particularly if previously poor metabolic
control is improved by intensified insulin therapy.
Paediatric population
In general, the safety profile for children and adolescents (≤ 18 years of age) is similar to the safety
profile for adults.
The adverse reaction reports received from post marketing surveillance included
relatively
more
frequent injection site reactions (injection site pain, injection site reaction) and skin reactions (rash,
urticaria) in children and adolescents (≤ 18 years of age) than in adults.
No clinical study safety data are available in children below 6 years of age.
Symptoms
Insulin overdose may lead to severe and sometimes long-term and life-threatening hypoglycaemia.
Management
Mild episodes of hypoglycaemia can usually be treated with oral carbohydrates. Adjustments in dose
of the medicinal product, meal patterns, or physical activity may be needed.
More severe episodes with coma, seizure, or neurologic impairment may be treated with
intramuscular/subcutaneous glucagon or concentrated intravenous glucose. Sustained carbohydrate
intake and observation may be necessary because hypoglycaemia may recur after apparent clinical
recovery.
5.
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Drugs used in diabetes. Insulins and analogues for injection, long-acting.
ATC Code: A10A E04.
Insulin glargine is a human insulin analogue designed to have a low solubility at neutral pH. It is
completely soluble at the acidic pH of the Lantus injection solution (pH 4). After injection into the
subcutaneous tissue, the acidic solution is neutralised leading to formation of micro-precipitates from
which small amounts of insulin glargine are continuously released, providing a smooth, peakless,
predictable concentration/time profile with a prolonged duration of action.
8
Insulin receptor binding: Insulin glargine is very similar to human insulin with respect to insulin
receptor binding kinetics. It can, therefore, be
considered to mediate the same type of effect via the
insulin receptor as insulin.
The primary activity of insulin, including insulin glargine, is regulation of glucose metabolism. Insulin
and its analogues lower blood glucose levels by stimulating peripheral glucose uptake, especially by
skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulin inhibits lipolysis in the
adipocyte, inhibits proteolysis and enhances protein synthesis.
In clinical pharmacology studies, intravenous insulin glargine and human insulin have been shown to
be equipotent when given at the same doses. As with all insulins, the time course of action of insulin
glargine may be affected by physical activity and other variables.
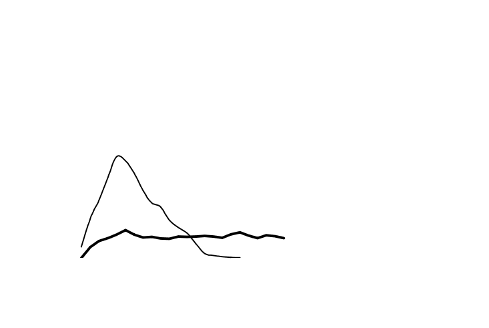
In euglycaemic clamp studies in healthy subjects or in patients with type 1 diabetes, the onset of action
of subcutaneous insulin glargine was slower than with human NPH insulin, its effect profile was
smooth and peakless, and the duration of its effect was prolonged.
The following graph shows the
results from a study in patients:
Activity Profile in Patients with Type 1 Diabetes
6
5
4
Insulin glargine
NPH insulin
3
2
1
0
0
10
20
30
Time (h) after s.c. injection
End of observation
period
*
determined as amount of glucose infused to maintain constant plasma glucose levels
(hourly mean values)
The longer duration of action of subcutaneous insulin glargine is directly related to its slower rate of
absorption and supports once daily administration. The time course of action of insulin and insulin
analogues such as insulin glargine may vary considerably in different individuals or within the same
individual.
In a clinical study, symptoms of hypoglycaemia or counter-regulatory hormone responses were similar
after intravenous insulin glargine and human insulin both in healthy volunteers and patients with
type 1 diabetes.
Effects of insulin glargine (once daily) on diabetic retinopathy were evaluated in an open-label 5 year
NPH-controlled study (NPH given bid) in 1024 type 2 diabetic patients in which progression of
retinopathy by 3 or more steps on the Early Treatment Diabetic Retinopathy Study (ETDRS) scale was
investigated by fundus photography. No significant difference was seen in the progression of diabetic
retinopathy when insulin glargine was compared to NPH insulin.
9




























Paediatric population
In a randomised, controlled clinical study, paediatric patients (age range 6 to 15 years) with type 1
diabetes (n = 349) were treated for 28 weeks with a basal-bolus insulin regimen where regular human
insulin was used before each meal. Insulin glargine was administered once daily at bedtime and NPH
human insulin was administered once or twice daily. Similar effects on glycohemoglobin and the
incidence of symptomatic hypoglycemia were observed in both treatment groups, however fasting
plasma glucose decreased more from baseline in the insulin glargine group than in the NPH group.
There was less severe hypoglycaemia in the insulin glargine group as well. One hundred forty three of
the patients treated with insulin glargine in this study continued treatment with insulin glargine in an
uncontrolled extension study with mean duration of follow-up of 2 years. No new safety signals were
seen during this extended treatment with insulin glargine.
A crossover study comparing insulin glargine plus lispro insulin to NPH plus regular human insulin
(each treatment administered for 16 weeks in random order) in 26 adolescent type 1 diabetic patients
aged 12 to 18 years was also performed. As in the paediatric study described above, fasting plasma
glucose reduction from baseline was greater in the insulin glargine group than in the NPH group.
HbA1c changes from baseline were similar between treatment groups; however blood glucose values
recorded overnight were significantly higher in the insulin glargine/ lispro group than the NPH/regular
group, with a mean nadir of 5.4 mM vs 4.1 mM. Correspondingly, the incidences of nocturnal
hypoglycaemia were 32 % in the insulin glargine / lispro group vs 52 % in the NPH / regular group.
5.2 Pharmacokinetic properties
In healthy subjects and diabetic patients, insulin serum concentrations indicated a slower and much
more prolonged absorption and showed a lack of a peak after subcutaneous injection of insulin
glargine in comparison to human NPH insulin. Concentrations were thus consistent with the time
profile of the pharmacodynamic activity of insulin glargine. The graph above shows the activity
profiles over time of insulin glargine and NPH insulin.
Insulin glargine injected once daily will reach steady state levels in 2-4 days after the first dose.
When given intravenously the elimination half-life of insulin glargine and human insulin were
comparable.
In man, insulin glargine is partly degraded in the subcutaneous tissue at the carboxyl terminus of the
Beta chain with formation of the active metabolites 21
A
-Gly-insulin and 21
A
-Gly-des-30
B
-Thr-insulin.
Unchanged insulin glargine and degradation products are also present in the plasma.
In clinical studies, subgroup analyses based on age and gender did not indicate any difference in safety
and efficacy in insulin glargine-treated patients compared to the entire study population.
Paediatric population
No specific pharmacokinetics study in children or adolescents was conducted.
5.3 Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of safety
pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction.
6.
6.1 List of excipients
5 ml vial
Zinc chloride,
m-cresol,
10
glycerol,
hydrochloric acid,
sodium hydroxide,
water for injections.
10 ml vial
Zinc chloride,
m-cresol,
glycerol,
hydrochloric acid,
polysorbate 20,
sodium hydroxide,
water for injections
6.2 Incompatibilities
This medicinal product must not be mixed with other medicinal products. It is important to ensure that
syringes do not contain traces of any other material.
6.3 Shelf-life
2 years.
Shelf-life after first use of the vial
The medicinal product may be stored for a maximum of 4 weeks not above 25°C and away from direct
heat or direct light. Keep the vial in the outer carton in order to protect from light.
It is recommended that the date of the first use from the vial be noted on the label.
6.4 Special precautions for storage
Unopened vials
Store in a refrigerator (2°C-8°C).
Do not freeze.
Do not put Lantus next to the freezer compartment or a freezer pack.
Keep the vial in the outer carton in order to protect from light.
Opened vials
For storage precautions, see section 6.3.
6.5 Nature and contents of container
5 ml solution in a vial (type 1 colourless glass) with a flanged cap (aluminium), a stopper
(chlorobutyl
rubber (type 1)) and a tear-off cap (polypropylene).
Packs of 1, 2, 5 and 10 vials are available.
10 ml solution in a vial (type 1 colourless glass) with a flanged cap (aluminium), (type 1, laminate of
polyisoprene and bromobutyl rubber) a stopper and a tear-off cap (polypropylene). Packs of 1 vial are
available.
Not all pack sizes may be marketed.
6.6 Special precautions for disposal and other handling
Inspect the vial before use. It must only be used if the solution is clear, colourless, with no solid
particles visible, and if it is of water-like consistency. Since Lantus is a solution, it does not require
resuspension before use.
11
Lantus must not be mixed with any other insulin or diluted. Mixing or diluting can change its
time/action profile and mixing can cause precipitation.
Insulin label must always be checked before each injection to avoid medication errors between insulin
glargine and other insulins. (see section 4.4)
7.
Sanofi-Aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany.
8.
EU/1/00/134/001-004
EU/1/00/134/012
9.
Date of first authorisation: 9 June 2000
Date of latest renewal: 9 June 2010
Detailed information on this medicinal product is available on the website of the European Medicines
Agency
http://www.ema.europa.eu
12
1.
Lantus 100 units/ml solution for injection in a cartridge.
2.
Each ml contains 100 units insulin glargine (equivalent to 3.64 mg).
Each cartridge contains 3 ml of solution for injection, equivalent to 300 units.
Insulin glargine is produced by recombinant DNA technology in
Escherichia coli
.
For a full list of excipients, see section 6.1.
3.
Solution for injection.
Clear colourless solution.
4.
For the treatment of adults, adolescents and children of 6 years or above with diabetes mellitus, where
treatment with insulin is required.
Posology
Lantus contains insulin glargine, an insulin analogue, and has a prolonged duration of action.
Lantus should be administered once daily at any time but at the same time each day.
The Lantus dose regimen (dose and timing) should be individually adjusted. In patients with type 2
diabetes mellitus, Lantus can also be given together with orally active antidiabetic medicinal products.
The potency of this medicinal product is stated in units. These units are exclusive to Lantus and are
not the same as IU or the units used to express the potency of other insulin analogues. (see section 5.1
).
Elderly population (≥ 65 years old)
In the elderly, progressive deterioration of renal function may lead to a steady decrease in insulin
requirements.
Renal impairment
In patients with renal impairment, insulin requirements may be diminished due to reduced insulin
metabolism.
Hepatic impairment
In patients with hepatic impairment, insulin requirements may be diminished due to reduced capacity
for gluconeogenesis and reduced insulin metabolism.
13
Paediatric population
Safety and efficacy of Lantus have been established in adolescents and children of 6 years and above.
In children, efficacy and safety of Lantus have only been demonstrated when given in the evening.
Due to limited experience on the efficacy and safety of Lantus in children below the age of 6 years,
Lantus should only be used in this age group undercareful medical supervision.
Transition from other insulins to Lantus
When changing from a treatment regimen with an intermediate or long-acting insulin to a regimen
with Lantus, a change of the dose of the basal insulin may be required and the concomitant
antidiabetic treatment may need to be adjusted (dose and timing of additional regular insulins or fast-
acting insulin analogues or the dose of oral antidiabetic medicinal products).
To reduce the risk of nocturnal and early morning hypoglycaemia, patients who are changing their
basal insulin regimen from a twice daily NPH insulin to a once daily regimen with Lantus should
reduce their daily dose of basal insulin by 20-30 % during the first weeks of treatment.
During the first weeks the reduction should, at least partially, be compensated by an increase in
mealtime insulin, after this period the regimen should be adjusted individually.
As with other insulin analogues, patients with high insulin doses because of antibodies to human
insulin may experience an improved insulin response with Lantus.
Close metabolic monitoring is recommended during the transition and in the initial weeks thereafter.
With improved metabolic control and resulting increase in insulin sensitivity a further adjustment in
dose regimen may become necessary. Dose adjustment may also be required, for example, if the
patient's weight or life-style changes, change of timing of insulin dose or other circumstances arise that
increase susceptibility to hypo-or hyperglycaemia (see section 4.4).
Method of administration
Lantus is administered subcutaneously.
Lantus should not be administered intravenously. The prolonged duration of action of Lantus is
dependent on its injection into subcutaneous tissue. Intravenous administration of the usual
subcutaneous dose could result in severe hypoglycaemia.
There are no clinically relevant differences in serum insulin or glucose levels after abdominal, deltoid
or thigh administration of Lantus. Injection sites must be rotated within a given injection area from one
injection to the next.
Lantus must not be mixed with any other insulin or diluted. Mixing or diluting can change its
time/action profile and mixing can cause precipitation.
For further details on handling, see section 6.6.
Hypersensitivity to the active substance or to any of the excipients.
14
Lantus is not the insulin of choice for the treatment of diabetic ketoacidosis. Instead, regular insulin
administered intravenously
is recommended in such cases.
In case of insufficient glucose control or a tendency to hyper- or hypoglycaemic episodes, the patient's
adherence to the prescribed treatment regimen, injection sites and proper injection technique and all
other relevant factors must be reviewed before dose adjustment is considered.
Transferring a patient to another type or brand of insulin should be done under strict medical
supervision. Changes in strength, brand (manufacturer), type (regular, NPH, lente, long-acting, etc.),
origin (animal, human, human insulin analogue) and/or method of manufacture may result in the need
for a change in dose.
Insulin administration may cause insulin antibodies to form. In rare cases, the presence of such insulin
antibodies may necessitate adjustment of the insulin dose in order to correct a tendency to hyper- or
hypoglycaemia. (see section 4.8)
Hypoglycaemia
The time of occurrence of hypoglycaemia depends on the action profile of the insulins used and may,
therefore, change when the treatment regimen is changed. Due to more sustained basal insulin supply
with Lantus, less nocturnal but more early morning hypoglycaemia can be expected.
Particular caution should be exercised, and intensified blood glucose monitoring is advisable in
patients in whom hypoglycaemic episodes might be of particular clinical relevance, such as in patients
with significant stenoses of the coronary arteries or of the blood vessels supplying the brain (risk of
cardiac or cerebral complications of hypoglycaemia) as well as in patients with proliferative
retinopathy, particularly if not treated with photocoagulation (risk of transient amaurosis following
hypoglycaemia).
Patients should be aware of circumstances where warning symptoms of hypoglycaemia are
diminished. The warning symptoms of hypoglycaemia may be changed, be less pronounced or be
absent in certain risk groups. These include patients:
- in whom glycaemic control is markedly improved,
- in whom hypoglycaemia develops gradually,
- who are elderly,
- after transfer from animal insulin to human insulin,
- in whom an autonomic neuropathy is present,
- with a long history of diabetes,
- suffering from a psychiatric illness,
- receiving concurrent treatment with certain other medicinal products (see section 4.5).
Such situations may result in severe hypoglycaemia (and possibly loss of consciousness) prior to the
patient's awareness of hypoglycaemia.
The prolonged effect of subcutaneous insulin glargine may delay recovery from hypoglycaemia.
If normal or decreased values for glycated haemoglobin are noted, the possibility of recurrent,
unrecognised (especially nocturnal) episodes of hypoglycaemia must be considered.
15
Adherence of the patient to
the dose and dietary regimen, correct insulin administration and awareness
of hypoglycaemia symptoms are essential to reduce the risk of hypoglycaemia. Factors increasing the
susceptibility to hypoglycaemia require particularly close monitoring and may necessitate dose
adjustment. These include:
-
change in the injection area,
-
improved insulin sensitivity (e.g., by removal of stress factors),
-
intercurrent illness (e.g. vomiting, diarrhoea),
-
inadequate food intake,
-
missed meals,
-
alcohol consumption,
-
certain uncompensated endocrine disorders, (e.g. in hypothyroidism and in anterior pituitary or
adrenocortical insufficiency),
-
concomitant treatment with certain other medicinal products.
Intercurrent illness
Intercurrent illness requires intensified metabolic monitoring. In many cases urine tests for ketones are
indicated, and often it is necessary to adjust the insulin dose. The insulin requirement is often
increased. Patients with type 1 diabetes must continue to consume at least a small amount of
carbohydrates on a regular basis, even if they are able to eat only little or no food, or are vomiting etc.
and they must never omit insulin entirely.
Pens to be used with Lantus cartridges
The Lantus cartridges should only be used with the following pens: OptiPen, ClikSTAR, Tactipen and
Autopen 24 and should not be used with any other reusable pen as the dosing accuracy has only been
established with the listed pens.
Medication errors
Medication errors have been reported in which other insulins, particularly short-acting insulins, have
been accidentally administered instead of insulin glargine. Insulin label must always be checked
before each injection to avoid medication errors between insulin glargine and other insulins.
Combination of Lantus with pioglitazone
Cases of cardiac failure have been reported when pioglitazone was used in combination with insulin,
especially in patients with risk factors for development of cardiac heart failure. This should be kept in
mind if treatment with the combination of pioglitazone and Lantus is considered. If the combination is
used, patients should be observed for signs and symptoms of heart failure, weight gain and oedema.
Pioglitazone should be discontinued if any deterioration in cardiac symptoms occurs.
A number of substances affect glucose metabolism and may require dose adjustment of insulin
glargine.
Substances that may enhance the blood-glucose-lowering effect and increase susceptibility to
hypoglycaemia include oral antidiabetic medicinal products, angiotensin converting enzyme (ACE)
inhibitors, disopyramide, fibrates, fluoxetine, monoamine oxidase (MAO) inhibitors, pentoxifylline,
propoxyphene, salicylates and sulfonamide antibiotics.
Substances that may reduce the blood-glucose-lowering effect include corticosteroids, danazol,
diazoxide, diuretics, glucagon, isoniazid, oestrogens and progestogens, phenothiazine derivatives,
somatropin, sympathomimetic medicinal products (e.g. epinephrine [adrenaline], salbutamol,
16
-
unaccustomed, increased or prolonged physical activity,
terbutaline), thyroid hormones, atypical antipsychotic medicinal products (e.g. clozapine and
olanzapine) and protease inhibitors.
Beta-blockers, clonidine, lithium salts or alcohol may either potentiate or weaken the blood-glucose-
lowering effect of insulin. Pentamidine may cause hypoglycaemia, which may sometimes be followed
by hyperglycaemia.
In addition, under the influence of sympatholytic medicinal products such as beta-blockers, clonidine,
guanethidine and reserpine, the signs of adrenergic counter-regulation may be reduced or absent.
Pregnancy
For insulin glargine no clinical data on exposed pregnancies from controlled clinical trials are
available. A moderate amount of data on pregnant women (between 300-1000 pregnancy outcomes)
exposed to marketed insulin glargine indicate no adverse effects of insulin glargine on pregnancy and
no malformative nor feto/neonatal toxicity of insulin glargine.
Animal data do not indicate reproductive toxicity.
The use of Lantus may be considered during pregnancy, if necessary.
It is essential for patients with pre-existing or gestational diabetes to maintain good metabolic control
throughout pregnancy. Insulin requirements may decrease during the first trimester and generally
increase during the second and third trimesters. Immediately after delivery, insulin requirements
decline rapidly (increased risk of hypoglycaemia). Careful monitoring of glucose control is essential.
Breastfeeding
It is unknown whether insulin glargine is excreted in human milk. No metabolic effects of ingested
insulin glargine on the breastfed newborn/infant are anticipated since insulin glargine as a peptide is
digested into aminoacids in the human gastrointestinal tract.
Breastfeeding women may require adjustments in insulin dose and diet.
Fertility
Animal studies do not indicate direct harmful effects with respect to fertility.
The patient's ability to concentrate and react may be impaired as a result of hypoglycaemia or
hyperglycaemia or, for example, as a result of visual impairment. This may constitute a risk in
situations where these abilities are of special importance (e.g. driving a car or operating machines).
Patients should be advised to take precautions to avoid hypoglycaemia whilst driving. This is
particularly important in those who have reduced or absent awareness of the warning symptoms of
hypoglycaemia or have frequent episodes of hypoglycaemia. It should be considered whether it is
advisable to drive or operate machines in these circumstances.
Hypoglycaemia, in general the most frequent adverse reaction of insulin therapy, may occur if the
insulin dose is too high in relation to the insulin requirement.
The following related adverse reactions from clinical investigations are listed below by system organ
class and in order of decreasing incidence (very common: ≥ 1/10; common: ≥ 1/100 to < 1/10;
uncommon: ≥ 1/1,000 to < 1/100; rare: ≥ 1/10,000 to < 1/1,000; very rare: < 1/10,000).
17
Within each frequency grouping, adverse reactions are presented in order of decreasing seriousnes
s.
MedDRA
system organ
classes
Very common Common
Uncommon Rare
Veryrare
Immune system
disorders
Allergic
reactions
Metabolism and
nutrition
disorders
Hypoglycaemia
Nervous system
disorders
Dysgeusia
Eyes disorders
Visual
impairment
Retinopathy
Skin and
subcutaneous
tissue disorders
Lipohypertro-
phy
Lipoatrophy
Musculoskeletal
and connective
tissue disorders
Myalgia
General
disorders and
administration
site conditions
Injection site
reactions
Oedema
Metabolism and nutrition disorders
Severe hypoglycaemic attacks, especially if recurrent, may lead to neurological damage. Prolonged or
severe hypoglycaemic episodes may be life-threatening.
In many patients, the signs and symptoms of neuroglycopenia are preceded by signs of adrenergic
counter-regulation. Generally, the greater and more rapid the decline in blood glucose, the more
marked is the phenomenon of counter-regulation and its symptoms.
Immune system disorders
Immediate-type allergic reactions to insulin are rare. Such reactions to insulin (including insulin
glargine) or the excipients may, for example, be associated with generalised skin reactions, angio-
oedema, bronchospasm, hypotension and shock, and may be life-threatening.
Insulin administration may cause insulin antibodies to form. In clinical studies, antibodies that cross-
react with human insulin and insulin glargine were observed with the same frequency in both NPH-
insulin and insulin glargine treatment groups. In rare cases, the presence of such insulin antibodies
may necessitate adjustment of the insulin dose in order to correct a tendency to hyper- or
hypoglycaemia.
Eyes disorders
A marked change in glycaemic control may cause temporary visual impairment, due to temporary
alteration in the turgidity and refractive index of the lens.
Long-term improved glycaemic control decreases the risk of progression of diabetic retinopathy.
However, intensification of insulin therapy with abrupt improvement in glycaemic control may be
associated with temporary worsening of diabetic retinopathy. In patients with proliferative retinopathy,
18














particularly if not treated with photocoagulation, severe hypoglycaemic episodes may result in
transient amaurosis.
Skin and subcutaneous tissue disorders
As with any insulin therapy, lipodystrophy may occur at the injection site and delay local insulin
absorption. Continuous rotation of the injection site within the given injection area may help to reduce
or prevent these reactions.
General disorders and administration site conditions
Injection site reactions include redness, pain, itching, hives, swelling, or inflammation. Most minor
reactions to insulins at the injection site usually resolve in a few days to a few weeks.
Rarely, insulin may cause sodium retention and oedema particularly if previously poor metabolic
control is improved by intensified insulin therapy.
Paediatric population
In general, the safety profile for children and adolescents (≤ 18 years of age) is similar to the safety
profile for adults.
The adverse reaction reports received from post marketing surveillance included
relatively
more
frequent injection site reactions (injection site pain, injection site reaction) and skin reactions (rash,
urticaria) in children and adolescents (≤ 18 years of age) than in adults.
No clinical study safety data are available in children below 6 years of age.
Symptoms
Insulin overdose may lead to severe and sometimes long-term and life-threatening hypoglycaemia.
Management
Mild episodes of hypoglycaemia can usually be treated with oral carbohydrates. Adjustments in dose
of the medicinal product, meal patterns, or physical activity may be needed.
More severe episodes with coma, seizure, or neurologic impairment may be treated with
intramuscular/subcutaneous glucagon or concentrated intravenous glucose. Sustained carbohydrate
intake and observation may be necessary because hypoglycaemia may recur after apparent clinical
recovery.
5.
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Drugs used in diabetes. Insulins and analogues for injection, long-acting.
ATC Code: A10A E04.
Insulin glargine is a human insulin analogue designed to have a low solubility at neutral pH. It is
completely soluble at the acidic pH of the Lantus injection solution (pH 4). After injection into the
subcutaneous tissue, the acidic solution is neutralised leading to formation of micro-precipitates from
which small amounts of insulin glargine are continuously released, providing a smooth, peakless,
predictable concentration/time profile with a prolonged duration of action.
19
Insulin receptor binding: Insulin glargine is very similar to human insulin with respect to insulin
receptor binding kinetics. It can, therefore, be
considered to mediate the same type of effect via the
insulin receptor as insulin.
The primary activity of insulin, including insulin glargine, is regulation of glucose metabolism. Insulin
and its analogues lower blood glucose levels by stimulating peripheral glucose uptake, especially by
skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulin inhibits lipolysis in the
adipocyte, inhibits proteolysis and enhances protein synthesis.
In clinical pharmacology studies, intravenous insulin glargine and human insulin have been shown to
be equipotent when given at the same doses. As with all insulins, the time course of action of insulin
glargine may be affected by physical activity and other variables.
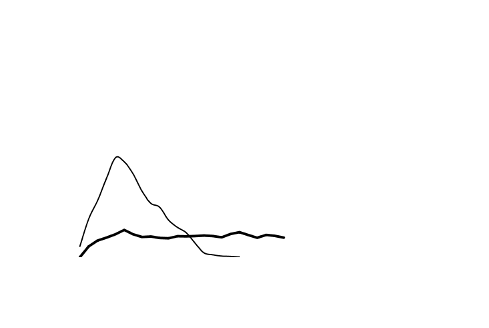
In euglycaemic clamp studies in healthy subjects or in patients with type 1 diabetes, the onset of action
of subcutaneous insulin glargine was slower than with human NPH insulin, its effect profile was
smooth and peakless, and the duration of its effect was prolonged.
The following graph shows the
results from a study in patients:
Figure 1. Activity Profile in Patients with Type 1 Diabetes
6
5
4
Insulin glargine
NPH insulin
3
2
1
0
0
10
20
30
Time (h) after s.c. injection
End of observation
period
*determined as amount of glucose infused to maintain constant plasma glucose levels (hourly mean
values)
The longer duration of action of subcutaneous insulin glargine is directly related to its slower rate of
absorption and supports once daily administration. The time course of action of insulin and insulin
analogues such as insulin glargine may vary considerably in different individuals or within the same
individual.
In a clinical study, symptoms of hypoglycaemia or counter-regulatory hormone responses were similar
after intravenous insulin glargine and human insulin both in healthy volunteers and patients with
type 1 diabetes.
Effects of insulin glargine (once daily) on diabetic retinopathy were evaluated in an open-label 5 year
NPH-controlled study (NPH given bid) in 1024 type 2 diabetic patients in which progression of
retinopathy by 3 or more steps on the Early Treatment Diabetic Retinopathy Study (ETDRS) scale was
investigated by fundus photography. No significant difference was seen in the progression of diabetic
retinopathy when insulin glargine was compared to NPH insulin.
20



























Paediatric population
In a randomised, controlled clinical study, paediatric patients (age range 6 to 15 years) with type 1
diabetes (n = 349) were treated for 28 weeks with a basal-bolus insulin regimen where regular human
insulin was used before each meal. Insulin glargine was administered once daily at bedtime and NPH
human insulin was administered once or twice daily. Similar effects on glycohemoglobin and the
incidence of symptomatic hypoglycemia were observed in both treatment groups, however fasting
plasma glucose decreased more from baseline in the insulin glargine group than in the NPH group.
There was less severe hypoglycaemia in the insulin glargine group as well. One hundred forty three of
the patients treated with insulin glargine in this study continued treatment with insulin glargine in an
uncontrolled extension study with mean duration of follow-up of 2 years. No new safety signals were
seen during this extended treatment with insulin glargine.
A crossover study comparing insulin glargine plus lispro insulin to NPH plus regular human insulin
(each treatment administered for 16 weeks in random order) in 26 adolescent type 1 diabetic patients
aged 12 to 18 years was also performed. As in the paediatric study described above, fasting plasma
glucose reduction from baseline was greater in the insulin glargine group than in the NPH group.
HbA1c changes from baseline were similar between treatment groups; however blood glucose values
recorded overnight were significantly higher in the insulin glargine/ lispro group than the NPH/regular
group, with a mean nadir of 5.4 mM vs 4.1 mM. Correspondingly, the incidences of nocturnal
hypoglycaemia were 32 % in the insulin glargine / lispro group vs 52 % in the NPH / regular group.
5.2 Pharmacokinetic properties
In healthy subjects and diabetic patients, insulin serum concentrations indicated a slower and much
more prolonged absorption and showed a lack of a peak after subcutaneous injection of insulin
glargine in comparison to human NPH insulin. Concentrations were thus consistent with the time
profile of the pharmacodynamic activity of insulin glargine. The graph above shows the activity
profiles over time of insulin glargine and NPH insulin.
Insulin glargine injected once daily will reach steady state levels in 2-4 days after the first dose.
When given intravenously the elimination half-life of insulin glargine and human insulin were
comparable.
In man, insulin glargine is partly degraded in the subcutaneous tissue at the carboxyl terminus of the
Beta chain with formation of the active metabolites 21
A
-Gly-insulin and 21
A
-Gly-des-30
B
-Thr-insulin.
Unchanged insulin glargine and degradation products are also present in the plasma.
In clinical studies, subgroup analyses based on age and gender did not indicate any difference in safety
and efficacy in insulin glargine-treated patients compared to the entire study population.
Paediatric population
No specific pharmacokinetic study in children or adolescents was conducted.
5.3 Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of safety
pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction.
6.
6.1 List of excipients
Zinc chloride, m-cresol, glycerol, hydrochloric acid, sodium hydroxide, water for injections.
21
6.2 Incompatibilities
This medicinal product must not be mixed with other medicinal products. It is important to ensure that
syringes do not contain traces of any other material.
6.3 Shelf life
3 years.
Shelf life after first use of the cartridge
The medicinal product may be stored for a maximum of 4 weeks not above 25°C and away from direct
heat or direct light. The pen containing a cartridge must not be stored in the refrigerator.
The pen cap must be put back on the pen after each injection in order to protect from light.
6.4 Special precautions for storage
Unopened cartridges
Store in a refrigerator (2°C-8°C).
Do not freeze.
Do not put Lantus next to the freezer compartment or a freezer pack.
Keep the cartridge in the outer carton in order to protect from light.
In use cartridges
For storage precautions, see section 6.3.
6.5 Nature and contents of container
3 ml solution in a cartridge (type 1 colourless glass) with a black plunger (bromobutyl rubber) and a
flanged cap (aluminium) with a stopper (bromobutyl or laminate of polyisoprene and bromobutyl
rubber). Packs of 1, 3, 4, 5, 6, 8, 9 and 10 cartridges are available. Not all pack sizes may be marketed.
6.6 Special precautions for disposal and other handling
Lantus must not be mixed with any other insulin or diluted. Mixing or diluting can change its
time/action profile and mixing can cause precipitation.
Insulin pen
The Lantus cartridges are to be used only in conjunction with OptiPen, ClikSTAR, Autopen 24 or
Tactipen (see section 4.4). Not all of these pens may be marketed in your country.
The pen should be used as recommended in the information provided by the device manufacturer.
The manufacturer’s instructions for using the pen must be followed carefully for loading the cartridge,
attaching the needle, and administering the insulin injection.
If the insulin pen is damaged or not working properly (due to mechanical defects) it has to be
discarded, and a new insulin pen has to be used.
If the pen malfunctions (see instructions for using the pen), the solution may be drawn from the
cartridge into a syringe (suitable for an insulin with 100 units/ml) and injected.
22
Cartridge
Before insertion into the pen, the cartridge must be stored at room temperature for 1 to 2 hours.
Inspect the cartridge before use. It must only be used if the solution is clear, colourless, with no solid
particles visible, and if it is of water-like consistency. Since Lantus is a solution, it does not require
resuspension before use.
Air bubbles must be removed from the cartridge before injection (see instructions for using the pen).
Empty cartridges must not be refilled.
Insulin label must always be checked before each injection to avoid medication errors between insulin
glargine and other insulins. (see section 4.4)
7.
Sanofi-Aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany
8.
EU/1/00/134/005-007
EU/1/00/134/013-017
9.
Date of first authorisation: 9 June 2000
Date of latest renewal: 9 June 2010
Detailed information on this medicinal product is available on the website of the European Medicines
Agency
http://www.ema.europa.eu
23
1.
Lantus 100 units/ml solution for injection in a cartridge for OptiClik.
2.
Each ml contains 100 units insulin glargine (equivalent to 3.64 mg).
Each cartridge contains 3 ml of solution for injection, equivalent to 300 units.
Insulin glargine is produced by recombinant DNA technology in
Escherichia coli
.
For a full list of excipients, see section 6.1.
3.
Solution for injection.
Clear colourless solution.
4.
For the treatment of adults, adolescents and children of 6 years or above with diabetes mellitus, where
treatment with insulin is required.
Posology
Lantus contains insulin glargine, an insulin analogue, and has a prolonged duration of action.
Lantus should be administered once daily at any time but at the same time each day.
The Lantus dose regimen (dose and timing) should be individually adjusted. In patients with type 2
diabetes mellitus, Lantus can also be given together with orally active antidiabetic medicinal products.
The potency of this medicinal product is stated in units. These units are exclusive to Lantus and are
not the same as IU or the units used to express the potency of other insulin analogues. (see
section 5.1).
Elderly population (≥ 65 years old)
In the elderly, progressive deterioration of renal function may lead to a steady decrease in insulin
requirements.
Renal impairment
In patients with renal impairment, insulin requirements may be diminished due to reduced insulin
metabolism.
Hepatic impairment
In patients with hepatic impairment, insulin requirements may be diminished due to reduced capacity
for gluconeogenesis and reduced insulin metabolism.
24
Paediatric population
Safety and efficacy of Lantus have been established in adolescents and children of 6 years and above.
In children, efficacy and safety of Lantus have only been demonstrated when given in the evening.
Due to limited experience on the efficacy and safety of Lantus in children below the age of 6 years,
Lantus should only be used in this age group under careful medical supervision.
Transition from other insulins to Lantus
When changing from a treatment regimen with an intermediate or long-acting insulin to a regimen
with Lantus, a change of the dose of the basal insulin may be required and the concomitant
antidiabetic treatment may need to be adjusted (dose and timing of additional regular insulins or fast-
acting insulin analogues or the dose of oral antidiabetic medicinal products).
To reduce the risk of nocturnal and early morning hypoglycaemia, patients who are changing their
basal insulin regimen from a twice daily NPH insulin to a once daily regimen with Lantus should
reduce their daily dose of basal insulin by 20-30 % during the first weeks of treatment.
During the first weeks the reduction should, at least partially, be compensated by an increase in
mealtime insulin, after this period the regimen should be adjusted individually.
As with other insulin analogues, patients with high insulin doses because of antibodies to human
insulin may experience an improved insulin response with Lantus.
Close metabolic monitoring is recommended during the transition and in the initial weeks thereafter.
With improved metabolic control and resulting increase in insulin sensitivity a further adjustment in
dose regimen may become necessary. Dose adjustment may also be required, for example, if the
patient's weight or life-style changes, change of timing of insulin dose or other circumstances arise that
increase susceptibility to hypo-or hyperglycaemia (see section 4.4).
Method of administration
Lantus is administered subcutaneously.
Lantus should not be administered intravenously. The prolonged duration of action of Lantus is
dependent on its injection into subcutaneous tissue. Intravenous administration of the usual
subcutaneous dose could result in severe hypoglycaemia.
There are no clinically relevant differences in serum insulin or glucose levels after abdominal, deltoid
or thigh administration of Lantus. Injection sites must be rotated within a given injection area from one
injection to the next.
Lantus must not be mixed with any other insulin or diluted. Mixing or diluting can change its
time/action profile and mixing can cause precipitation.
For further details on handling, see section 6.6.
Hypersensitivity to the active substance or to any of the excipients.
25
Lantus is not the insulin of choice for the treatment of diabetic ketoacidosis. Instead, regular insulin
administered intravenously
is recommended in such cases.
In case of insufficient glucose control or a tendency to hyper- or hypoglycaemic episodes, the patient's
adherence to the prescribed treatment regimen, injection sites and proper injection technique and all
other relevant factors must be reviewed before dose adjustment is considered.
Transferring a patient to another type or brand of insulin should be done under strict medical
supervision. Changes in strength, brand (manufacturer), type (regular, NPH, lente, long-acting, etc.),
origin (animal, human, human insulin analogue) and/or method of manufacture may result in the need
for a change in dose.
Insulin administration may cause insulin antibodies to form. In rare cases, the presence of such insulin
antibodies may necessitate adjustment of the insulin dose in order to correct a tendency to hyper- or
hypoglycaemia. (see section 4.8)
Hypoglycaemia
The time of occurrence of hypoglycaemia depends on the action profile of the insulins used and may,
therefore, change when the treatment regimen is changed. Due to more sustained basal insulin supply
with Lantus, less nocturnal but more early morning hypoglycaemia can be expected.
Particular caution should be exercised, and intensified blood glucose monitoring is advisable in
patients in whom hypoglycaemic episodes might be of particular clinical relevance, such as in patients
with significant stenoses of the coronary arteries or of the blood vessels supplying the brain (risk of
cardiac or cerebral complications of hypoglycaemia) as well as in patients with proliferative
retinopathy, particularly if not treated with photocoagulation (risk of transient amaurosis following
hypoglycaemia).
Patients should be aware of circumstances where warning symptoms of hypoglycaemia are
diminished. The warning symptoms of hypoglycaemia may be changed, be less pronounced or be
absent in certain risk groups. These include patients:
- in whom glycaemic control is markedly improved,
- in whom hypoglycaemia develops gradually,
- who are elderly,
- after transfer from animal insulin to human insulin,
- in whom an autonomic neuropathy is present,
- with a long history of diabetes,
- suffering from a psychiatric illness,
- receiving concurrent treatment with certain other medicinal products (see section 4.5).
Such situations may result in severe hypoglycaemia (and possibly loss of consciousness) prior to the
patient's awareness of hypoglycaemia.
The prolonged effect of subcutaneous insulin glargine may delay recovery from hypoglycaemia.
If normal or decreased values for glycated haemoglobin are noted, the possibility of recurrent,
unrecognised (especially nocturnal) episodes of hypoglycaemia must be considered.
26
Adherence of the patient to
the dose and dietary regimen, correct insulin administration and awareness
of hypoglycaemia symptoms are essential to reduce the risk of hypoglycaemia. Factors increasing the
susceptibility to hypoglycaemia require particularly close monitoring and may necessitate dose
adjustment. These include:
-
change in the injection area,
-
improved insulin sensitivity (e.g., by removal of stress factors),
-
intercurrent illness (e.g. vomiting, diarrhoea),
-
inadequate food intake,
-
missed meals,
-
alcohol consumption,
-
certain uncompensated endocrine disorders, (e.g. in hypothyroidism and in anterior pituitary or
adrenocortical insufficiency),
-
concomitant treatment with certain other medicinal products.
Intercurrent illness
Intercurrent illness requires intensified metabolic monitoring. In many cases urine tests for ketones are
indicated, and often it is necessary to adjust the insulin dose. The insulin requirement is often
increased. Patients with type 1 diabetes must continue to consume at least a small amount of
carbohydrates on a regular basis, even if they are able to eat only little or no food, or are vomiting etc.
and they must never omit insulin entirely.
Medication errors
Medication errors have been reported in which other insulins, particularly short-acting insulins, have
been accidentally administered instead of insulin glargine. Insulin label must always be checked
before each injection to avoid medication errors between insulin glargine and other insulins.
Combination of Lantus with pioglitazone
Cases of cardiac failure have been reported when pioglitazone was used in combination with insulin,
especially in patients with risk factors for development of cardiac heart failure. This should be kept in
mind if treatment with the combination of pioglitazone and Lantus is considered. If the combination is
used, patients should be observed for signs and symptoms of heart failure, weight gain and oedema.
Pioglitazone should be discontinued if any deterioration in cardiac symptoms occurs.
A number of substances affect glucose metabolism and may require dose adjustment of insulin
glargine.
Substances that may enhance the blood-glucose-lowering effect and increase susceptibility to
hypoglycaemia include oral antidiabetic medicinal products, angiotensin converting enzyme (ACE)
inhibitors, disopyramide, fibrates, fluoxetine, monoamine oxidase (MAO) inhibitors, pentoxifylline,
propoxyphene, salicylates and sulfonamide antibiotics.
Substances that may reduce the blood-glucose-lowering effect include corticosteroids, danazol,
diazoxide, diuretics, glucagon, isoniazid, oestrogens and progestogens, phenothiazine derivatives,
somatropin, sympathomimetic medicinal products (e.g. epinephrine [adrenaline], salbutamol,
terbutaline), thyroid hormones, atypical antipsychotic medicinal products (e.g. clozapine and
olanzapine) and protease inhibitors.
Beta-blockers, clonidine, lithium salts or alcohol may either potentiate or weaken the blood-glucose-
lowering effect of insulin. Pentamidine may cause hypoglycaemia, which may sometimes be followed
by hyperglycaemia.
27
-
unaccustomed, increased or prolonged physical activity,
In addition, under the influence of sympatholytic medicinal products such as beta-blockers, clonidine,
guanethidine and reserpine, the signs of adrenergic counter-regulation may be reduced or absent.
Pregnancy
For insulin glargine no clinical data on exposed pregnancies from controlled clinical trials are
available A moderate amount of data on pregnant women (between 300-1000 pregnancy outcomes)
exposed to marketed insulin glargine indicate no adverse effects of insulin glargine on pregnancy and
no malformative nor feto/neonatal toxicity of insulin glargine.
Animal data do not indicate reproductive toxicity.
The use of Lantus may be considered during pregnancy, if necessary.
It is essential for patients with pre-existing or gestational diabetes to maintain good metabolic control
throughout pregnancy. Insulin requirements may decrease during the first trimester and generally
increase during the second and third trimesters. Immediately after delivery, insulin requirements
decline rapidly (increased risk of hypoglycaemia). Careful monitoring of glucose control is essential.
Breastfeeding
It is unknown whether insulin glargine is excreted in human milk. No metabolic effects of ingested
insulin glargine on the breastfed newborn/infant are anticipated since insulin glargine as a peptide is
digested into aminoacids in the human gastrointestinal tract.
Breastfeeding women may require adjustments in insulin dose and diet.
Fertility
Animal studies do not indicate direct harmful effects with respect to fertility.
The patient's ability to concentrate and react may be impaired as a result of hypoglycaemia or
hyperglycaemia or, for example, as a result of visual impairment. This may constitute a risk in
situations where these abilities are of special importance (e.g. driving a car or operating machines).
Patients should be advised to take precautions to avoid hypoglycaemia whilst driving. This is
particularly important in those who have reduced or absent awareness of the warning symptoms of
hypoglycaemia or have frequent episodes of hypoglycaemia. It should be considered whether it is
advisable to drive or operate machines in these circumstances.
Hypoglycaemia, in general the most frequent adverse reaction of insulin therapy, may occur if the
insulin dose is too high in relation to the insulin requirement.
The following related adverse reactions from clinical investigations are listed below by system organ
class and in order of decreasing incidence (very common: ≥ 1/10; common: ≥ 1/100 to < 1/10;
uncommon: ≥ 1/1,000 to < 1/100; rare: ≥ 1/10,000 to < 1/1,000; very rare: < 1/10,000).
28
Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness.
MedDRA
system organ
classes
Very common Common
Uncommon Rare
Veryrare
Immune system
disorders
Allergic
reactions
Metabolism and
nutrition
disorders
Hypoglycaemia
Nervous system
disorders
Dysgeusia
Eyes disorders
Visual
impairment
Retinopathy
Skin and
subcutaneous
tissue disorders
Lipohypertro--
phy
Lipoatrophy
Musculoskeletal
and connective
tissue disorders
Myalgia
General
disorders and
administration
site conditions
Injection site
reactions
Oedema
Metabolism and nutrition disorders
Severe hypoglycaemic attacks, especially if recurrent, may lead to neurological damage. Prolonged or
severe hypoglycaemic episodes may be life-threatening.
In many patients, the signs and symptoms of neuroglycopenia are preceded by signs of adrenergic
counter-regulation. Generally, the greater and more rapid the decline in blood glucose, the more
marked is the phenomenon of counter-regulation and its symptoms.
Immune system disorders
Immediate-type allergic reactions to insulin are rare. Such reactions to insulin (including insulin
glargine) or the excipients may, for example, be associated with generalised skin reactions, angio-
oedema, bronchospasm, hypotension and shock, and may be life-threatening.
Insulin administration may cause insulin antibodies to form. In clinical studies, antibodies that cross-
react with human insulin and insulin glargine were observed with the same frequency in both NPH-
insulin and insulin glargine treatment groups. In rare cases, the presence of such insulin antibodies
may necessitate adjustment of the insulin dose in order to correct a tendency to hyper- or
hypoglycaemia.
Eyes disorders
A marked change in glycaemic control may cause temporary visual impairment, due to temporary
alteration in the turgidity and refractive index of the lens.
Long-term improved glycaemic control decreases the risk of progression of diabetic retinopathy.
However, intensification of insulin therapy with abrupt improvement in glycaemic control may be
29















associated with temporary worsening of diabetic retinopathy. In patients with proliferative retinopathy,
particularly if not treated with photocoagulation, severe hypoglycaemic episodes may result in
transient amaurosis.
Skin and subcutaneous tissue disorders
As with any insulin therapy, lipodystrophy may occur at the injection site and delay local insulin
absorption. Continuous rotation of the injection site within the given injection area may help to reduce
or prevent these reactions.
General disorders and administration site conditions
Injection site reactions include redness, pain, itching, hives, swelling, or inflammation. Most minor
reactions to insulins at the injection site usually resolve in a few days to a few weeks.
Rarely, insulin may cause sodium retention and oedema particularly if previously poor metabolic
control is improved by intensified insulin therapy.
Paediatric population
In general, the safety profile for children and adolescents (≤ 18 years of age) is similar to the safety
profile for adults.
The adverse reaction reports received from post marketing surveillance included
relatively
more
frequent injection site reactions (injection site pain, injection site reaction) and skin reactions (rash,
urticaria) in children and adolescents (≤ 18 years of age) than in adults.
No clinical study safety data are available in children below 6 years of age.
Symptoms
Insulin overdose may lead to severe and sometimes long-term and life-threatening hypoglycaemia.
Management
Mild episodes of hypoglycaemia can usually be treated with oral carbohydrates. Adjustments in dose
of the medicinal product, meal patterns, or physical activity may be needed.
More severe episodes with coma, seizure, or neurologic impairment may be treated with
intramuscular/subcutaneous glucagon or concentrated intravenous glucose. Sustained carbohydrate
intake and observation may be necessary because hypoglycaemia may recur after apparent clinical
recovery.
5.
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Drugs used in diabetes. Insulins and analogues for injection, long-acting.
ATC Code: A10A E04.
Insulin glargine is a human insulin analogue designed to have a low solubility at neutral pH. It is
completely soluble at the acidic pH of the Lantus injection solution (pH 4). After injection into the
subcutaneous tissue, the acidic solution is neutralised leading to formation of micro-precipitates from
which small amounts of insulin glargine are continuously released, providing a smooth, peakless,
predictable concentration/time profile with a prolonged duration of action.
30
Insulin receptor binding: Insulin glargine is very similar to human insulin with respect to insulin
receptor binding kinetics. It can, therefore, be
considered to mediate the same type of effect via the
insulin receptor as insulin.
The primary activity of insulin, including insulin glargine, is regulation of glucose metabolism. Insulin
and its analogues lower blood glucose levels by stimulating peripheral glucose uptake, especially by
skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulin inhibits lipolysis in the
adipocyte, inhibits proteolysis and enhances protein synthesis.
In clinical pharmacology studies, intravenous insulin glargine and human insulin have been shown to
be equipotent when given at the same doses. As with all insulins, the time course of action of insulin
glargine may be affected by physical activity and other variables.
In euglycaemic clamp studies in healthy subjects or in patients with type 1 diabetes, the onset of action
of subcutaneous insulin glargine was slower than with human NPH insulin, its effect profile was
smooth and peakless, and the duration of its effect was prolonged.
The following graph shows the
results from a study in patients:
Figure 1. Activity Profile in Patients with Type 1 Diabetes
6
5
4
Insulin glargine
NPH insulin
3
2
1
0
0
10
20
30
Time (h) after s.c. injection
End of observation
period
*determined as amount of glucose infused to maintain constant plasma glucose levels (hourly mean
values)
The longer duration of action of subcutaneous insulin glargine is directly related to its slower rate of
absorption and supports once daily administration. The time course of action of insulin and insulin
analogues such as insulin glargine may vary considerably in different individuals or within the same
individual.
In a clinical study, symptoms of hypoglycaemia or counter-regulatory hormone responses were similar
after intravenous insulin glargine and human insulin both in healthy volunteers and patients with
type 1 diabetes.
Effects of insulin glargine (once daily) on diabetic retinopathy were evaluated in an open-label 5 year
NPH-controlled study (NPH given bid) in 1024 type 2 diabetic patients in which progression of
retinopathy by 3 or more steps on the Early Treatment Diabetic Retinopathy Study (ETDRS) scale was
investigated by fundus photography. No significant difference was seen in the progression of diabetic
retinopathy when insulin glargine was compared to NPH insulin.
31
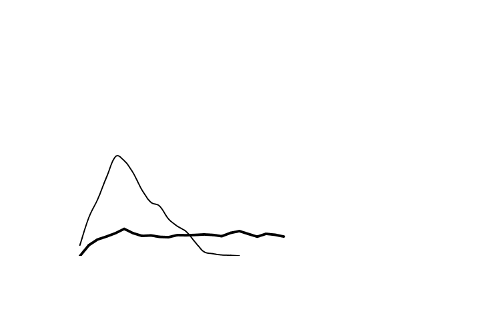



























Paediatric population
In a randomised, controlled clinical study, paediatric patients (age range 6 to 15 years) with type 1
diabetes (n = 349) were treated for 28 weeks with a basal-bolus insulin regimen where regular human
insulin was used before each meal. Insulin glargine was administered once daily at bedtime and NPH
human insulin was administered once or twice daily. Similar effects on glycohemoglobin and the
incidence of symptomatic hypoglycemia were observed in both treatment groups, however fasting
plasma glucose decreased more from baseline in the insulin glargine group than in the NPH group.
There was less severe hypoglycaemia in the insulin glargine group as well. One hundred forty three of
the patients treated with insulin glargine in this study continued treatment with insulin glargine in an
uncontrolled extension study with mean duration of follow-up of 2 years. No new safety signals were
seen during this extended treatment with insulin glargine.
A crossover study comparing insulin glargine plus lispro insulin to NPH plus regular human insulin
(each treatment administered for 16 weeks in random order) in 26 adolescent type 1 diabetic patients
aged 12 to 18 years was also performed. As in the paediatric study described above, fasting plasma
glucose reduction from baseline was greater in the insulin glargine group than in the NPH group.
HbA1c changes from baseline were similar between treatment groups; however blood glucose values
recorded overnight were significantly higher in the insulin glargine/ lispro group than the NPH/regular
group, with a mean nadir of 5.4 mM vs 4.1 mM. Correspondingly, the incidences of nocturnal
hypoglycaemia were 32 % in the insulin glargine / lispro group vs 52 % in the NPH / regular group.
5.2 Pharmacokinetic properties
In healthy subjects and diabetic patients, insulin serum concentrations indicated a slower and much
more prolonged absorption and showed a lack of a peak after subcutaneous injection of insulin
glargine in comparison to human NPH insulin. Concentrations were thus consistent with the time
profile of the pharmacodynamic activity of insulin glargine. The graph above shows the activity
profiles over time of insulin glargine and NPH insulin.
Insulin glargine injected once daily will reach steady state levels in 2-4 days after the first dose.
When given intravenously the elimination half-life of insulin glargine and human insulin were
comparable.
In man, insulin glargine is partly degraded in the subcutaneous tissue at the carboxyl terminus of the
Beta chain with formation of the active metabolites 21
A
-Gly-insulin and 21
A
-Gly-des-30
B
-Thr-insulin.
Unchanged insulin glargine and degradation products are also present in the plasma.
In clinical studies, subgroup analyses based on age and gender did not indicate any difference in safety
and efficacy in insulin glargine-treated patients compared to the entire study population.
Paediatric population
No specific pharmacokinetic study in children or adolescents was conducted.
5.3 Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of safety
pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction.
6.
6.1 List of excipients
Zinc chloride, m-cresol, glycerol, hydrochloric acid, sodium hydroxide, water for injections.
32
6.2 Incompatibilities
This medicinal product must not be mixed with other medicinal products. It is important to ensure that
syringes do not contain traces of any other material.
6.3 Shelf life
3 years.
Shelf life after first use of the cartridge
The medicinal product may be stored for a maximum of 4 weeks not above 25°C and away from direct
heat or direct light. The pen containing a cartridge must not be stored in the refrigerator.
The pen cap must be put back on the pen after each injection in order to protect from light.
6.4 Special precautions for storage
Unopened cartridges
Store in a refrigerator (2°C-8°C).
Do not freeze.
Do not put Lantus next to the freezer compartment or a freezer pack.
Keep the cartridge in the outer carton in order to protect from light.
In use cartridges
For storage precautions, see section 6.3.
6.5 Nature and contents of container
3 ml solution in a cartridge (type 1 colourless glass) with a black plunger (bromobutyl rubber) and a
flanged cap (aluminium) with a stopper (bromobutyl or laminate of polyisoprene and bromobutyl
rubber). The glass cartridge is irreversibly integrated in a transparent container and assembled to a
plastic mechanism with a threaded rod at one extremity.
Packs of 1, 3, 4, 5, 6, 8, 9 and 10 cartridges for OptiClik are available. Not all pack sizes may be
marketed.
6.6 Special precautions for disposal and other handling
Lantus must not be mixed with any other insulin or diluted. Mixing or diluting can change its
time/action profile and mixing can cause precipitation.
The cartridges for OptiClik are to be used in conjunction with OptiClik only and as recommended in the
information provided by the device manufacturer.
The manufacturer’s instructions for using the pen must be followed carefully for loading the cartridge,
attaching the needle, and administering the insulin injection.
If OptiClik is damaged or not working properly (due to mechanical defects) it has to be discarded, and
a new OptiClik has to be used.
Before insertion into the pen, the cartridge must be stored at room temperature for 1 to 2 hours.
Inspect the cartridge before use. It must only be used if the cartridge is intact and the solution is clear,
colourless, with no solid particles visible, and if it is of water-like consistency. Since Lantus is a solution, it
does not require resuspension before use.
Air bubbles must be removed from the cartridge before injection (see instructions for using the pen).
Empty cartridges must not be refilled.
If the pen malfunctions (see instructions for using the pen), the solution may be drawn from the
cartridge into a syringe (suitable for an insulin with 100 units/ml) and injected.
33
Insulin label must always be checked before each injection to avoid medication errors between insulin
glargine and other insulins. (see section 4.4)
7.
Sanofi-Aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany
8.
EU/1/00/134/022-029
9.
Date of first authorisation: 9 June 2000
Date of latest renewal: 9 June 2010
Detailed information on this medicinal product is available on the website of the European Medicines
Agency
http://www.ema.europa.eu
34
1.
FURTHER INFORMATION
What Lantus contains
-
The active substance is insulin glargine. Each millilitre of the solution contains 100 units of the
active substance insulin glargine (equivalent to 3.64 mg).
-
Other ingredients of Lantus are: zinc chloride, m-cresol, glycerol, sodium hydroxide,
hydrochloric acid and water for injections.
What Lantus looks like and contents of the pack
Lantus SoloStar 100 units/ml solution for injection in a pre-filled pen, is a clear and colourless
solution.
Each pen
contains 3 ml of solution for injection (equivalent to 300 units). Packs of 1, 3, 4, 5, 6, 8, 9
and 10 pre-filled pens of 3 ml are available. Not all pack sizes may be marketed.
Marketing Authorisation Holder and Manufacturer
Marketing Authorization Holder
Sanofi-Aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany.
Manufacturer
Sanofi-Aventis Deutschland GmbH,
D-65926 Frankfurt am Main,
Germany.
Aventis Pharma (Sanofi-aventis group)
Rainham Road South
Dagenham, Essex RM10 7XS
United Kingdom
149

For any information about this medicine, please contact the local representative of the Marketing
Authorisation Holder.
België/Belgique/Belgien
sanofi-aventis Belgium
Tél/Tel: +32 (0)2 710 54 00
Luxembourg/Luxemburg
sanofi-aventis Belgium
Tél/Tel: +32 (0)2 710 54 00 (Belgique/Belgien)
България
sanofi-aventis Bulgaria EOOD
Тел.: +359 (0)2 970 53 00
Magyarország
sanofi-aventis zrt., Magyarország
Tel.: +36 1 505 0050
Česká republika
sanofi-aventis, s.r.o.
Tel: +420 233 086 111
Malta
sanofi-aventis Malta Ltd.
Tel: +356 21493022
Danmark
sanofi-aventis Denmark A/S
Tlf: +45 45 16 70 00
Nederland
sanofi-aventis Netherlands B.V.
Tel: +31 (0)182 557 755
Deutschland
Sanofi-Aventis Deutschland GmbH
Tel: +49 (0)180 2 222010
Norge
sanofi-aventis Norge AS
Tlf: +47 67 10 71 00
Eesti
sanofi-aventis Estonia OÜ
Tel: +372 627 34 88
Österreich
sanofi-aventis GmbH
Tel: +43 1 80 185 – 0
Ελλάδα
sanofi-aventis AEBE
Τηλ: +30 210 900 16 00
Polska
sanofi-aventis Sp. z o.o.
Tel.: +48 22 280 00 00
España
sanofi-aventis, S.A
Tel: +34 93 485 94 00
Portugal
sanofi-aventis - Produtos Farmacêuticos, Lda.
Tel: +351 21 35 89 400
France
sanofi-aventis France
Tél: 0 800 222 555
Appel depuis l’étranger : +33 1 57 63 23 23
România
sanofi-aventis România S.R.L.
Tel: +40 (0) 21 317 31 36
Ireland
sanofi-aventis Ireland Ltd.
Tel: +353 (0) 1 403 56 00
Slovenija
sanofi-aventis d.o.o.
Tel: +386 1 560 48 00
Ísland
Vistor hf.
Sími: +354 535 7000
Slovenská republika
sanofi-aventis Pharma Slovakia s.r.o.
Tel: +421 2 33 100 100
Italia
sanofi-aventis S.p.A.
Tel: 800 13 12 12 (domande di tipo tecnico)
+39 02 393 91 (altre domande e chiamate
dall'estero)
Suomi/Finland
sanofi-aventis Oy
Puh/Tel: +358 (0) 201 200 300
150
Κύπρος
sanofi-aventis Cyprus Ltd.
Τηλ: +357 22 871600
Sverige
sanofi-aventis AB
Tel: +46 (0)8 634 50 00
Latvija
sanofi-aventis Latvia SIA
Tel: +371 67 33 24 51
United Kingdom
sanofi-aventis
Tel: +44 (0) 1483 505 515
Lietuva
UAB sanofi-aventis Lietuva
Tel: +370 5 2755224
This leaflet was last approved on
Detailed information on this medicine is available on the European Medicines Agency web site:
http://www.ema.europa.eu/
151
HYPERGLYCAEMIA AND HYPOGLYCAEMIA
Always carry some sugar (at least 20 grams) with you.
Carry some information with you to show you are diabetic.
HYPERGLYCAEMIA (high blood sugar levels)
If your blood sugar is too high (hyperglycaemia), you may not have injected enough insulin.
Why does hyperglycaemia occur?
Examples include:
-
you have not injected your insulin or not injected enough, or if it has become less effective,for
example through incorrect storage,
-
your insulin pen does not work properly,
-
you are doing less exercise than usual, you are under stress (emotional distress, excitement), or
you have an injury, operation, infection or fever,
-
you are taking or have taken certain other medicines (see section 2, "Using other medicines").
Warning symptoms of hyperglycaemia
Thirst, increased need to urinate, tiredness, dry skin, reddening of the face, loss of appetite, low blood
pressure, fast heart beat, and glucose and ketone bodies in urine . Stomach pain, fast and deep
breathing, sleepiness or even loss of consciousness may be signs of a serious condition (ketoacidosis)
resulting from lack of insulin.
What should you do if you experience hyperglycaemia?
Test your blood sugar level and your urine for ketones as soon as any of the above symptoms
occur
. Severe hyperglycaemia or ketoacidosis must always be treated by a doctor, normally in a
hospital.
HYPOGLYCAEMIA (low blood sugar levels)
If your blood sugar level falls too much you may become unconscious. Serious hypoglycaemia may
cause a heart attack or brain damage and may be life-threatening. You normally should be able to
recognise when your blood sugar is falling too much so that you can take the right actions.
Why does hypoglycaemia occur?
Examples include:
-
you inject too much insulin,
-
you miss meals or delay them,
-
you do not eat enough, or eat food containing less carbohydrate than normal (sugar and
substances similar to sugar are called carbohydrates; however, artificial sweeteners are NOT
carbohydrates),
-
you lose carbohydrates due to vomiting or diarrhoea,
-
you are doing more exercise than usual or a different type of physical activity,
-
you are recovering from an injury or operation or other stress,
-
you are recovering from an illness or from fever,
-
you are taking or have stopped taking certain other medicines (see section 2, "Using other
medicines").
152
-
you drink alcohol, particularly if you are not eating much,



Hypoglycaemia is also more likely to occur if
-
you have just begun insulin treatment or changed to another insulin preparation (when changing
from your previous basal insulin to Lantus hypoglycaemia, if it occurs, may be more likely to
occur in the morning than at night),
-
your blood sugar levels are almost normal or are unstable,
-
you change the area of skin where you inject insulin (for example from the thigh to the upper
arm),
-
you suffer from severe kidney or liver disease, or some other disease such as hypothyroidism.
Warning symptoms of hypoglycaemia
- In your body
Examples of symptoms that tell you that your blood sugar level is falling too much or too fast :
sweating, clammy skin, anxiety, fast heart beat, high blood pressure, palpitations and irregular
heartbeat,. These symptoms often develop before the symptoms of a low sugar level in the brain.
- In your brain
Examples of symptoms that indicate a low sugar level in the brain: headaches, intense hunger, nausea,
vomiting, tiredness, sleepiness, sleep disturbances, restlessness, aggressive behaviour, lapses in
concentration, impaired reactions, depression, confusion, speech disturbances (sometimes total loss of
speech), visual disorders, trembling, paralysis, tingling sensations (paraesthesia), numbness and
tingling sensations in the area of the mouth, dizziness, loss of self-control, inability to look after
yourself, convulsions, loss of consciousness.
The first symptoms which alert you to hypoglycaemia ("warning symptoms") may change, be weaker
or may be missing altogether if
-
you are elderly, if you have had diabetes for a long time or if you suffer from a certain type of
nervous disease (diabetic autonomic neuropathy),
-
you have recently suffered hypoglycaemia (for example the day before) or if it develops slowly,
-
you have recently changed from an animal insulin to a human insulin such as Lantus,
-
you are taking or have taken certain other medicines (see section 2, "Using other medicines").
In such a case, you may develop severe hypoglycaemia (and even faint) before you are aware of the
problem. Be familiar with your warning symptoms. If necessary, more frequent blood sugar testing
can help to identify mild hypoglycaemic episodes that might otherwise be overlooked. If you are not
confident about recognising your warning symptoms, avoid situations (such as driving a car) in which
you or others would be put at risk by hypoglycaemia.
What should you do if you experience hypoglycaemia?
1.
Do not inject insulin. Immediately take about 10 to 20 g sugar, such as glucose, sugar cubes or a
sugar-sweetened beverage. Caution: Artificial sweeteners and foods with artificial sweeteners
(such as diet drinks) are of no help in treating hypoglycaemia.
2.
Then eat something that has a long-acting effect in raising your blood sugar (such as bread or
pasta). Your doctor or nurse should have discussed this with you previously.
The recovery of hypoglycaemia may be delayed because Lantus has a long action.
3.
If the hypoglycaemia comes back again take another 10 to 20 g sugar.
4.
Speak to a doctor immediately if you are not able to control the hypoglycaemia or if it recurs.
153
-
you have almost normal or, at least, greatly improved blood sugar levels,



Tell your relatives, friends and close colleagues the following:
If you are not able to swallow or if you are unconscious, you will require an injection of glucose or
glucagon (a medicine which increases blood sugar). These injections are justified even if it is not
certain that you have hypoglycaemia.
It is advisable to test your blood sugar immediately after taking glucose to check that you really have
hypoglycaemia.
154



LANTUS solution for injection in a pre-filled pen. SoloStar. Instructions for use
SoloStar is a pre-filled pen for the injection of insulin.Your healthcare professional has decided that
SoloStar is right for you. Talk with your healthcare professional about proper injection technique
before using SoloStar.
Read these instructions carefully before using your SoloStar. If you are not able to follow all the
instructions completely on your own, use SoloStar only if you have help from a person who is able to
follow the instructions. Hold the pen as shown in this leaflet. To ensure that you read the dose
correctly, hold the pen horizontally, with the needle on the left and the dosage selector to the right as
shown in the illustrations below.
You can set doses from 1 to 80 units in steps of 1 unit. Each pen contains multiple doses.
Keep this leaflet for future reference.
If you have any questions about SoloStar or about diabetes, ask your healthcare professional or call the
local sanofi-aventis number on the front of this leaflet.
Schematic diagram of the pen
Important information for use of SoloStar:
Always attach a new needle before each use. Only use needles that are compatible for use with
SoloStar.
Always perform the safety test before each injection (see Step 3).
This pen is only for your use. Do not share it with anyone else.
If your injection is given by another person, special caution must be taken by this person to
avoid accidental needle injury and transmission of infection.
Never use SoloStar if it is damaged or if you are not sure that it is working properly.
Always have a spare SoloStar in case your SoloStar is lost or damaged.
Step 1. Check the insulin
A
. Check the label on your SoloStar to make sure you have the correct insulin. The Lantus Solostar
is grey with a purple injection button.
B.
Take off the pen cap.
C.
Check the appearance of your insulin. Lantus is a clear insulin. Do not use this SoloStar if the
insulin is cloudy, coloured or has particles.
155

Step 2. Attach the needle
Always use a new sterile needle for each injection. This helps prevent contamination, and potential
needle blocks.
A
. Remove the protective seal from a new needle.
B.
Line up the needle with the pen, and keep it straight as you attach it (screw or push on,
depending on the needle type).
If the needle is not kept straight while you attach it, it can damage the rubber seal and cause
leakage, or break the needle.
Step 3. Perform a Safety test
Always perform the safety test before each injection. This ensures that you get an accurate dose by:
ensuring that pen and needle work properly
removing air bubbles
A
. Select a dose of 2 units by turning the dosage selector.
B.
Take off the outer needle cap and keep it to remove the used needle after injection. Take off the
inner needle cap and discard it.
C.
Hold the pen with the needle pointing upwards.
D.
Tap the insulin reservoir so that any air bubbles rise up towards the needle.
156

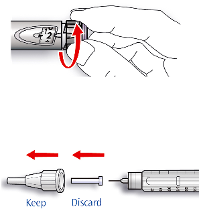
E.
Press the injection button all the way in. Check if insulin comes out of the needle tip.
You may have to perform the safety test several times before insulin is seen.
If no insulin comes out, check for air bubbles and repeat the safety test two more times to
remove them.
If still no insulin comes out, the needle may be blocked. Change the needle and try again.
If no insulin comes out after changing the needle, your SoloStar may be damaged. Do not use
this SoloStar.
Step 4. Select the dose
You can set the dose in steps of 1 unit, from a minimum of 1 unit to a maximum of 80 units. If you
need a dose greater than 80 units, you should give it as two or more injections.
A
. Check that the dose window shows “0” following the safety test.
B
. Select your required dose (in the example below, the selected dose is 30 units). If you turn past
your dose, you can turn back down.
Do not push the injection button while turning, as insulin will come out.
You cannot turn the dosage selector past the number of units left in the pen. Do not force the
dosage selector to turn. In this case, either you can inject what is remaining in the pen and
complete your dose with a new SoloStar or use a new SoloStar for your full dose.
Step 5. Inject the dose
A
. Use the injection method as instructed by your healthcare professional.
B
. Insert the needle into the skin.
157

C
. Deliver the dose by pressing the injection button in all the way. The number in the dose window
will return to “0” as you inject.
D
. Keep the injection button pressed all the way in. Slowly count to 10 before you withdraw the
needle from the skin. This ensures that the full dose will be delivered.
The pen plunger moves with each dose. The plunger will reach the end of the cartridge when the
total of 300 units of insulin has been used.
Step 6. Remove and discard the needle
Always remove the needle after each injection and store SoloStar without a needle attached.
This helps prevent:
Contamination and/or infection,
Entry of air into the insulin reservoir and leakage of insulin, which can cause inaccurate dosing.
A
. Put the outer needle cap back on the needle, and use it to unscrew the needle from the pen. To
reduce the risk of accidental needle injury, never replace the inner needle cap.
If your injection is given by another person, or if you are giving an injection to another person,
special caution must be taken by this person when removing and disposing of the needle.
Follow recommended safety measures for removal and disposal of needles (contact your health
care professional) in order to reduce the risk of accidental needle injury and transmission of
infectious diseases.
B.
Dispose of the needle safely, as instructed by your healthcare professional.
C
. Always put the pen cap back on the pen, then store the pen until your next injection.
Storage Instructions
Please check the reverse (insulin) side of this leaflet for instructions on how to store SoloStar.
If your SoloStar is in cool storage, take it out 1 to 2 hours before you inject to allow it to warm up.
Cold insulin is more painful to inject.
Discard your used SoloStar as required by your local authorities.
Maintenance
Protect your SoloStar from dust and dirt.
You can clean the outside of your SoloStar by wiping it with a damp cloth.
Do not soak, wash or lubricate the pen as this may damage it.
Your SoloStar is designed to work accurately and safely. It should be handled with care. Avoid
situations where SoloStar might be damaged. If you are concerned that your SoloStar may be
damaged, use a new one.
158

Source: European Medicines Agency
 - Please bookmark this page (add it to your favorites).
- Please bookmark this page (add it to your favorites).
- If you wish to link to this page, you can do so by referring to the URL address below this line.
https://theodora.com/drugs/eu/lantus.html
Copyright © 1995-2021 ITA all rights reserved.