| DRUGS INDEX | MANUFACTURERS INDEX | ANATOMY | GEOGRAPHY | USA STATISTICS | CHINA STATISTICS | RELIGION | JOBS |
 |
||
Evista Tablets (Lilly) | ||
|
- Drugs index - Manufacturers - Feedback 
|
DESCRIPTIONEVISTA® (raloxifene hydrochloride) is a selective estrogen receptor modulator (SERM) that belongs to the benzothiophene class of compounds. The chemical structure is:
The chemical designation is methanone, [6-hydroxy-2-(4-hydroxyphenyl)benzo[ b ]thien-3-yl]-[4-[2-(1-piperidinyl)ethoxy]phenyl]-, hydrochloride. Raloxifene hydrochloride (HCl) has the empirical formula C 28 H 27 NO 4 S·HCl, which corresponds to a molecular weight of 510.05. Raloxifene HCl is an off-white to pale-yellow solid that is very slightly soluble in water. EVISTA is supplied in a tablet dosage form for oral administration. Each EVISTA tablet contains 60 mg of raloxifene HCl, which is the molar equivalent of 55.71 mg of free base. Inactive ingredients include anhydrous lactose, carnauba wax, crospovidone, FD&C Blue No. 2 aluminum lake, hypromellose, lactose monohydrate, magnesium stearate, modified pharmaceutical glaze, polyethylene glycol, polysorbate 80, povidone, propylene glycol, and titanium dioxide.
CLINICAL PHARMACOLOGYMechanism of ActionDecreases in estrogen levels after oophorectomy or menopause lead to increases in bone resorption and accelerated bone loss. Bone is initially lost rapidly because the compensatory increase in bone formation is inadequate to offset resorptive losses. In addition to loss of estrogen, this imbalance between resorption and formation may be due to age-related impairment of osteoblasts or their precursors. In some women, these changes will eventually lead to decreased bone mass, osteoporosis, and increased risk for fractures, particularly of the spine, hip, and wrist. Vertebral fractures are the most common type of osteoporotic fracture in postmenopausal women. The biological actions of raloxifene are largely mediated through binding to estrogen receptors. This binding results in activation of certain estrogenic pathways and blockade of others. Thus, raloxifene is a SERM. Raloxifene decreases resorption of bone and reduces biochemical markers of bone turnover to the premenopausal range. These effects on bone are manifested as reductions in the serum and urine levels of bone turnover markers, decreases in bone resorption based on radiocalcium kinetics studies, increases in bone mineral density (BMD), and decreases in incidence of fractures. Raloxifene also has effects on lipid metabolism. Raloxifene decreases total and LDL cholesterol levels but does not increase triglyceride levels ( see PRECAUTIONS ). It does not change total HDL cholesterol levels. Preclinical data demonstrate that raloxifene is an estrogen antagonist in uterine and breast tissues. Clinical trial data (through a median of 42 months) suggest that EVISTA lacks estrogen-like effects on the uterus and breast tissue. PharmacokineticsThe disposition of raloxifene has been evaluated in more than 3000 postmenopausal women in selected raloxifene osteoporosis treatment and prevention clinical trials using a population approach. Pharmacokinetic data were also obtained in conventional pharmacology studies in 292 postmenopausal women. Raloxifene exhibits high within-subject variability (approximately 30% coefficient of variation) of most pharmacokinetic parameters. Table 1 summarizes the pharmacokinetic parameters of raloxifene. Absorption Raloxifene is absorbed rapidly after oral administration. Approximately 60% of an oral dose is absorbed, but presystemic glucuronide conjugation is extensive. Absolute bioavailability of raloxifene is 2.0%. The time to reach average maximum plasma concentration and bioavailability are functions of systemic interconversion and enterohepatic cycling of raloxifene and its glucuronide metabolites. Administration of raloxifene HCl with a standardized, high-fat meal increases the absorption of raloxifene (C max 28% and AUC 16%), but does not lead to clinically meaningful changes in systemic exposure. EVISTA can be administered without regard to meals.
Distribution Following oral administration of single doses ranging from 30 to 150 mg of raloxifene HCl, the apparent volume of distribution is 2348 L/kg and is not dose dependent. Raloxifene and the monoglucuronide conjugates are highly (95%) bound to plasma proteins. Raloxifene binds to both albumin and (alpha)1-acid glycoprotein, but not to sex-steroid binding globulin.
Metabolism Biotransformation and disposition of raloxifene in humans have been determined following oral administration of 14 C-labeled raloxifene. Raloxifene undergoes extensive first-pass metabolism to the glucuronide conjugates: raloxifene-4'-glucuronide, raloxifene-6-glucuronide, and raloxifene-6, 4'-diglucuronide. No other metabolites have been detected, providing strong evidence that raloxifene is not metabolized by cytochrome P450 pathways. Unconjugated raloxifene comprises less than 1% of the total radiolabeled material in plasma. The terminal log-linear portions of the plasma concentration curves for raloxifene and the glucuronides are generally parallel. This is consistent with interconversion of raloxifene and the glucuronide metabolites. Following intravenous administration, raloxifene is cleared at a rate approximating hepatic blood flow. Apparent oral clearance is 44.1 L/kg·hr. Raloxifene and its glucuronide conjugates are interconverted by reversible systemic metabolism and enterohepatic cycling, thereby prolonging its plasma elimination half-life to 27.7 hours after oral dosing. Results from single oral doses of raloxifene predict multiple-dose pharmacokinetics. Following chronic dosing, clearance ranges from 40 to 60 L/kg·hr. Increasing doses of raloxifene HCl (ranging from 30 to 150 mg) result in slightly less than a proportional increase in the area under the plasma time concentration curve (AUC).
Excretion Raloxifene is primarily excreted in feces, and less than 0.2% is excreted unchanged in urine. Less than 6% of the raloxifene dose is eliminated in urine as glucuronide conjugates.
Special PopulationsGeriatric --No differences in raloxifene pharmacokinetics were detected with regard to age (range 42 to 84 years). Pediatric --The pharmacokinetics of raloxifene have not been evaluated in a pediatric population. Gender --Total extent of exposure and oral clearance, normalized for lean body weight, are not significantly different between age-matched female and male volunteers. Race --Pharmacokinetic differences due to race have been studied in 1712 women including 97.5% Caucasian, 1.0% Asian, 0.7% Hispanic, and 0.5% Black in the osteoporosis treatment trial and in 1053 women including 93.5% Caucasian, 4.3% Hispanic, 1.2% Asian, and 0.5% Black in the osteoporosis prevention trials. There were no discernible differences in raloxifene plasma concentrations among these groups; however, the influence of race cannot be conclusively determined. Renal Insufficiency --Since negligible amounts of raloxifene are eliminated in urine, a study in patients with renal insufficiency was not conducted. In the osteoporosis treatment and prevention trials, raloxifene and metabolite concentrations in women with estimated creatinine clearance as low as 21 mL/min are similar to women with normal creatinine clearance. Hepatic Dysfunction --Raloxifene was studied, as a single dose, in Child-Pugh Class A patients with cirrhosis and total serum bilirubin ranging from 0.6 to 2.0 mg/dL. Plasma raloxifene concentrations were approximately 2.5 times higher than in controls and correlated with bilirubin concentrations. Safety and efficacy have not been evaluated further in patients with hepatic insufficiency ( see WARNINGS ). Drug-Drug InteractionsClinically significant drug-drug interactions are discussed in PRECAUTIONS. Ampicillin and Amoxicillin --Peak concentrations of raloxifene and the overall extent of absorption are reduced 28% and 14%, respectively, with co-administration of ampicillin. These reductions are consistent with decreased enterohepatic cycling associated with antibiotic reduction of enteric bacteria. However, the systemic exposure and the elimination rate of raloxifene were not affected. Therefore, EVISTA can be concurrently administered with ampicillin. In the osteoporosis treatment trial, co-administration of amoxicillin had no discernible differences in plasma raloxifene concentrations. Antacids --Concurrent administration of calcium carbonate or aluminum and magnesium hydroxide-containing antacids does not affect the systemic exposure of raloxifene. Corticosteroids --The chronic administration of raloxifene in postmenopausal women has no effect on the pharmacokinetics of methylprednisolone given as a single oral dose. Cholestyramine --See PRECAUTIONS . Cyclosporine --The co-administration of EVISTA with cyclosporine has not been evaluated. Digoxin --Raloxifene has no effect on the pharmacokinetics of digoxin. Warfarin --See PRECAUTIONS .
ANIMAL PHARMACOLOGYThe skeletal effects of raloxifene treatment were assessed in ovariectomized rats and monkeys. In rats, raloxifene prevented increased bone resorption and bone loss after ovariectomy. There were positive effects of raloxifene on bone strength, but the effects varied with time. Cynomolgus monkeys were treated with raloxifene or conjugated estrogens for 2 years. In terms of bone cycles, this is equivalent to approximately 6 years in humans. Raloxifene and estrogen suppressed bone turnover, and increased BMD in the lumbar spine and in the central cancellous bone of the proximal tibia. In this animal model, there was a positive correlation between vertebral compressive breaking force and BMD of the lumbar spine. Histologic examination of bone from rats and monkeys treated with raloxifene showed no evidence of woven bone, marrow fibrosis, or mineralization defects. These results are consistent with data from human studies of radiocalcium kinetics and markers of bone metabolism, and are consistent with the action of EVISTA as a skeletal antiresorptive agent.
CLINICAL STUDIESIn postmenopausal women with osteoporosis, EVISTA reduced the risk of vertebral fractures. EVISTA also increased BMD of the spine, hip, and total body. Similarly, in early postmenopausal women without osteoporosis (women with normal or low BMD without fracture), EVISTA increased spine, hip, and total body BMD relative to calcium alone at 24 months. The effect on hip bone mass was similar to that for the spine. Treatment of OsteoporosisThe effects of EVISTA on fracture incidence and BMD in postmenopausal women with osteoporosis were examined at 3 years in a large randomized, placebo-controlled, double-blind multinational osteoporosis treatment trial. All vertebral fractures were diagnosed radiographically; some of these fractures also were associated with symptoms (i.e., clinical fractures). The study population consisted of 7705 postmenopausal women with osteoporosis as defined by: a) low BMD (vertebral or hip BMD at least 2.5 standard deviations below the mean value for healthy young women) without baseline vertebral fractures, or b) one or more baseline vertebral fractures. Women enrolled in this study had a median age of 67 years (range 31 to 80) and a median time since menopause of 19 years. EVISTA, 60 mg administered once daily, increased spine and hip BMD by 2 to 3%. EVISTA decreased the incidence of the first vertebral fracture from 4.3% for placebo to 1.9% for EVISTA (relative risk reduction = 55%) and subsequent vertebral fractures from 20.2% for placebo to 14.1% for EVISTA (relative risk reduction = 30%) (Table 2). All women in the study received calcium (500 mg/day) and vitamin D (400 to 600 IU/day). EVISTA reduced the incidence of vertebral fractures whether or not patients had a vertebral fracture upon study entry. The decrease in incidence of vertebral fracture was greater than could be accounted for by increase in BMD alone.
The mean percentage change in BMD from baseline for EVISTA was statistically significantly greater than for placebo at each skeletal site (Table 3).
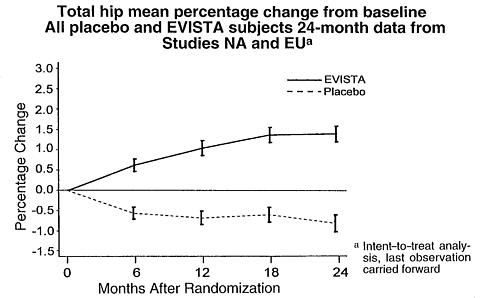
Discontinuation from the study was required when excessive bone loss or multiple incident vertebral fractures occurred. Such discontinuation was statistically significantly more frequent in the placebo group (3.7%) than in the EVISTA group (1.1%). Prevention of OsteoporosisThe effects of EVISTA on BMD in postmenopausal women were examined in three randomized, placebo-controlled, double-blind osteoporosis prevention trials: (1) a North American trial enrolled 544 women; (2) a European trial, 601 women; and (3) an international trial, 619 women who had undergone hysterectomy. In these trials, all women received calcium supplementation (400 to 600 mg/day). Women enrolled in these studies had a median age of 54 years and a median time since menopause of 5 years (less than 1 year up to 15 years postmenopause). The majority of the women were Caucasian (93.5%). Women were included if they had spine BMD between 2.5 standard deviations below and 2 standard deviations above the mean value for healthy young women. The mean T scores (number of standard deviations above or below the mean in healthy young women) for the three studies ranged from -1.01 to -0.74 for spine BMD and included women both with normal and low BMD. EVISTA, 60 mg administered once daily, produced increases in bone mass vs. calcium supplementation alone, as reflected by dual-energy x-ray absorptiometric (DXA) measurements of hip, spine, and total body BMD. Compared with placebo, the increases in BMD for each of the three studies were statistically significant at 12 months and were maintained at 24 months (Table 4). The placebo groups lost approximately 1% of BMD over 24 months.
EVISTA also increased BMD compared with placebo in the total body by 1.3% to 2.0% and in Ward's Triangle (hip) by 3.1% to 4.0%. The effects of EVISTA on forearm BMD were inconsistent between studies. In Study EU, EVISTA prevented bone loss at the ultradistal radius, whereas in Study NA, it did not.
Assessments of Bone TurnoverIn a 31-week, open-label, radiocalcium kinetics study, 33 early postmenopausal women were randomized to treatment with once-daily EVISTA 60 mg, cyclic estrogen/progestin (0.625 mg conjugated estrogens daily with 5 mg medroxyprogesterone acetate daily for the first 2 weeks of each month [HRT]), or no treatment. Treatment with either EVISTA or HRT was associated with reduced bone resorption and a positive shift in calcium balance (-82 mg Ca/day and +60 mg Ca/day, respectively, for EVISTA and -162 mg Ca/day and +91 mg Ca/day, respectively, for HRT). In both the osteoporosis treatment and prevention trials, EVISTA therapy resulted in consistent, statistically significant suppression of bone resorption and bone formation, as reflected by changes in serum and urine markers of bone turnover (e.g., bone-specific alkaline phosphatase, osteocalcin, and collagen breakdown products). The suppression of bone turnover markers was evident by 3 months and persisted throughout the 36-month and 24-month observation periods. Bone HistomorphometryIn the treatment study, bone biopsies for qualitative and quantitative histomorphometry were obtained at baseline and after 2 years of treatment. There were 56 paired biopsies evaluable for all indices. In EVISTA-treated patients, there were statistically significant decreases in bone formation rate per tissue volume, consistent with a reduction in bone turnover. Normal bone quality was maintained; specifically, there was no evidence of osteomalacia, marrow fi-brosis, cellular toxicity, or woven bone after 2 years of treatment. The tissue- and cellular-level effects of raloxifene were assessed by histomorphometric evaluation of human iliac crest bone biopsies taken after administration of a fluorochrome substance to label areas of mineralizing bone. The effects of EVISTA on bone histomorphometry were determined by pre- and post-treatment biopsies in a 6-month study of Caucasian postmenopausal women who received once-daily doses of EVISTA 60 mg or 0.625 mg conjugated estrogens. Ten raloxifene-treated and eight estrogen-treated women had evaluable bone biopsies at baseline and after 6 months of therapy. Bone formation rate/bone volume and activation frequency, the primary efficacy parameters, decreased to a greater extent with conjugated estrogen treatment vs. EVISTA treatment, although the differences were not statistically significant. Bone in EVISTA- and estrogen-treated women showed no evidence of mineralization defects, woven bone, or marrow fibrosis. Effects on Lipid MetabolismThe effects of EVISTA on selected lipid fractions and clotting factors were evaluated in a 6-month study of 390 postmenopausal women. EVISTA was compared with oral continuous combined estrogen/progestin (0.625 mg conjugated estrogens plus 2.5 mg medroxyprogesterone acetate, [HRT]) and placebo (Table 5). EVISTA decreased serum total and LDL cholesterol without effects on serum total HDL cholesterol or triglycerides. In addition, EVISTA statistically significantly decreased serum fibrinogen and lipoprotein (a).
Consistent with results from the 6-month study, in the osteoporosis treatment (36 months) and prevention (24 months) studies, EVISTA statistically significantly decreased serum total and LDL cholesterol by 5% to 6% and 8% to 10%, respectively, compared to placebo. EVISTA did not affect HDL cholesterol or triglyceride levels. The effect of EVISTA-induced reductions in total and LDL cholesterol on risk for cardiovascular disease is currently under study. Effects on the UterusIn the osteoporosis treatment trial, endometrial thickness was evaluated annually in a subset of the study population (1781 patients) for 3 years. Placebo-treated women had a 0.27 mm mean decrease from baseline in endometrial thickness over 3 years, whereas the EVISTA-treated women had a 0.06 mm mean increase. Patients in the osteoporosis treatment study were not screened at baseline or excluded for pre-existing endometrial or uterine disease. This study was not specifically designed to detect endometrial polyps. Over the 36 months of the study, clinically or histologically benign endometrial polyps were reported in 17 of 1999 placebo-treated women, 37 of 1948 EVISTA-treated women, and in 31 of 2010 women treated with raloxifene HCl 120 mg/day. There was no difference between EVISTA- and placebo-treated women in the incidences of endometrial carcinoma, vaginal bleeding, or vaginal discharge. In placebo-controlled osteoporosis prevention trials, endometrial thickness was evaluated every 6 months (for 24 months) by transvaginal ultrasonography (TVU). A total of 2978 TVU measurements were collected from 831 women in all dose groups. Placebo-treated women had a 0.04 mm mean increase from baseline in endometrial thickness over 2 years, whereas the EVISTA-treated women had a 0.09 mm mean increase. Endometrial thickness measurements in raloxifene-treated women were indistinguishable from placebo. There were no differences between the raloxifene and placebo groups with respect to the incidence of reported vaginal bleeding. In a 6-month study of 18 postmenopausal women that compared EVISTA to conjugated estrogens (0.625 mg/day [ERT]), endpoint endometrial biopsies demonstrated stimulatory effects of ERT, which were not observed for EVISTA. All samples from EVISTA-treated women showed nonproliferative endometria. A 12-month study of uterine effects compared a higher dose of raloxifene HCl (150 mg/day) with HRT. At baseline, 43 raloxifene-treated postmenopausal women and 37 HRT-treated women had a nonproliferative endometrium. At study completion, endometria in all of the raloxifene-treated women remained nonproliferative whereas 13 HRT-treated women had developed proliferative changes. Also, HRT significantly increased uterine volume; raloxifene did not increase uterine volume. Thus, no stimulatory effect of raloxifene on the endometrium was detected at more than twice the recommended dose. Compared to placebo, EVISTA did not increase the risk of ovarian carcinoma. Effects on the BreastAcross all placebo-controlled trials, EVISTA was indistinguishable from placebo with regard to frequency and severity of breast pain and tenderness. EVISTA was associated with significantly less breast pain and tenderness than reported by women receiving estrogens with or without added progestin ( see ADVERSE REACTIONS and Table 6 ). Mammograms were routinely performed on an annual or biennial basis in all placebo-controlled clinical trials lasting at least 12 months. Independent review has determined that 25 cases (raloxifene and placebo combined) represented newly-diagnosed invasive breast cancer. Among 7108 women randomized to raloxifene, there were 10 cases of invasive breast cancer per 19,381 person-years of follow-up (0.52 per 1000). Among 3467 women randomized to placebo, there were 15 cases of invasive breast cancer per 9250 person-years of follow-up (1.62 per 1000). The effectiveness of raloxifene in reducing the risk of breast cancer has not been established.
INDICATIONS AND USAGEEVISTA is indicated for the treatment and prevention of osteoporosis in postmenopausal women. For either osteoporosis treatment or prevention, supplemental calcium and/or vitamin D should be added to the diet if daily intake is inadequate. Postmenopausal osteoporosis may be diagnosed by history or radiographic documentation of osteoporotic fracture, bone mineral densitometry, or physical signs of vertebral crush fractures (e.g., height loss, dorsal kyphosis). No single clinical finding or test result can quantify risk of postmenopausal osteoporosis with certainty. However, clinical assessment can help to identify women at increased risk. Widely accepted risk factors include Caucasian or Asian descent, slender body build, early estrogen deficiency, smoking, alcohol consumption, low calcium diet, sedentary lifestyle, and family history of osteoporosis. Evidence of increased bone turnover from serum and urine markers and low bone mass (e.g., at least 1 standard deviation below the mean for healthy, young adult women) as determined by densitometric techniques are also predictive. The greater the number of clinical risk factors, the greater the probability of developing postmenopausal osteoporosis.
CONTRAINDICATIONSEVISTA is contraindicated in lactating women or women who are or may become pregnant. EVISTA may cause fetal harm when administered to a pregnant woman. In rabbit studies, abortion and a low rate of fetal heart anomalies (ventricular septal defects) occurred in rabbits at doses >/=0.1 mg/kg (>/=0.04 times the human dose based on surface area, mg/m 2 ), and hydrocephaly was observed in fetuses at doses >/=10 mg/kg (>/=4 times the human dose based on surface area, mg/m 2 ). In rat studies, retardation of fetal development and developmental abnormalities (wavy ribs, kidney cavitation) occurred at doses >/=1 mg/kg (>/=0.2 times the human dose based on surface area, mg/m 2 ). Treatment of rats at doses of 0.1 to 10 mg/kg (0.02 to 1.6 times the human dose based on surface area, mg/m 2 ) during gestation and lactation produced effects that included delayed and disrupted parturition; decreased neonatal survival and altered physical development; sex- and age-specific reductions in growth and changes in pituitary hormone content; and decreased lymphoid compartment size in offspring. At 10 mg/kg, raloxifene disrupted parturition which resulted in maternal and progeny death and morbidity. Effects in adult offspring (4 months of age) included uterine hypoplasia and reduced fertility; however, no ovarian or vaginal pathology was observed. The patient should be apprised of the potential hazard to the fetus if this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug. EVISTA is contraindicated in women with active or past history of venous thromboembolic events, including deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis. EVISTA is contraindicated in women known to be hypersensitive to raloxifene or other constituents of the tablets.
WARNINGSVenous Thromboembolism --In clinical trials, EVISTA-treated women had an increased risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism). Other venous thromboembolic events could also occur. A less serious event, superficial thrombophlebitis, also has been reported more frequently with EVISTA. The greatest risk for deep vein thrombosis and pulmonary embolism occurs during the first 4 months of treatment, and the magnitude of risk appears to be similar to the reported risk associated with use of hormone replacement therapy. Because immobilization increases the risk for venous thromboembolic events independent of therapy, EVISTA should be discontinued at least 72 hours prior to and during prolonged immobilization (e.g., post-surgical recovery, prolonged bed rest), and EVISTA therapy should be resumed only after the patient is fully ambulatory. In addition, women taking EVISTA should be advised to move about periodically during prolonged travel. The risk-benefit balance should be considered in women at risk of thromboembolic disease for other reasons, such as congestive heart failure, superficial thrombophlebitis, and active malignancy. Premenopausal Use --There is no indication for premenopausal use of EVISTA. Safety of EVISTA in premenopausal women has not been established and its use is not recommended ( see CONTRAINDICATIONS ). Hepatic Dysfunction --Raloxifene was studied, as a single dose, in Child-Pugh Class A patients with cirrhosis and serum total bilirubin ranging from 0.6 to 2.0 mg/dL. Plasma raloxifene concentrations were approximately 2.5 times higher than in controls and correlated with total bilirubin concentrations. Safety and efficacy have not been evaluated further in patients with severe hepatic insufficiency.
PRECAUTIONSGeneralConcurrent Estrogen Therapy --The concurrent use of EVISTA and systemic estrogen or hormone replacement therapy (ERT or HRT) has not been studied in prospective clinical trials and therefore concomitant use of EVISTA with systemic estrogens is not recommended. Lipid Metabolism --EVISTA lowers serum total and LDL cholesterol by 6% to 11%, but does not affect serum concentrations of total HDL cholesterol or triglycerides. These effects should be taken into account in therapeutic decisions for patients who may require therapy for hyperlipidemia. Limited clinical data suggest that some women with a history of marked hypertriglyceridemia (>5.6 mmol/L or >500 mg/dL) in response to treatment with oral estrogen or estrogen plus progestin may develop increased levels of tri-glycerides when treated with EVISTA. Women with this medical history should have serum triglycerides monitored when taking EVISTA. Concurrent use of EVISTA and lipid-lowering agents has not been studied. Endometrium --EVISTA has not been associated with endometrial proliferation ( see Clinical Studies and ADVERSE REACTIONS ). Unexplained uterine bleeding should be investigated as clinically indicated. Breast --EVISTA has not been associated with breast enlargement, breast pain, or an increased risk of breast cancer ( see Clinical Studies and ADVERSE REACTIONS ). Any unexplained breast abnormality occurring during EVISTA therapy should be investigated. History of Breast Cancer --EVISTA has not been adequately studied in women with a prior history of breast cancer. Use in Men --Safety and efficacy have not been evaluated in men. Information for PatientsFor safe and effective use of EVISTA, the physician should inform patients about the following: Patient Immobilization --EVISTA should be discontinued at least 72 hours prior to and during prolonged immobilization (e.g., post-surgical recovery, prolonged bed rest), and patients should be advised to avoid prolonged restrictions of movement during travel because of the increased risk of venous thromboembolic events. Hot Flashes or Flushes --EVISTA may increase the incidence of hot flashes and is not effective in reducing hot flashes or flushes associated with estrogen deficiency. In some asymptomatic patients, hot flashes may occur upon beginning EVISTA therapy. Other Osteoporosis Treatment and Prevention Measures --Patients should be instructed to take supplemental calcium and/or vitamin D, if daily dietary intake is inadequate. Weight-bearing exercise should be considered along with the modification of certain behavioral factors, such as cigarette smoking, and/or alcohol consumption, if these factors exist. Physicians should instruct their patients to read the patient package insert before starting therapy with EVISTA and to re-read it each time the prescription is renewed. Drug InteractionsCholestyramine --Cholestyramine, an anion exchange resin, causes a 60% reduction in the absorption and enterohepatic cycling of raloxifene after a single dose. Co-administration of cholestyramine with EVISTA is not recommended. Although not specifically studied, it is anticipated that other anion exchange resins would have a similar effect. Warfarin --In vitro, raloxifene did not interact with the binding of warfarin. The co-administration of EVISTA and warfarin, a coumarin derivative, has been assessed in a single-dose study. In this study, raloxifene had no effect on the pharmacokinetics of warfarin. However, a 10% decrease in prothrombin time was observed in the single-dose study. If EVISTA is given concurrently with warfarin or other coumarin derivatives, prothrombin time should be monitored more closely when starting or stopping therapy with EVISTA. In the osteoporosis treatment trial, there were no clinically relevant effects of warfarin co-administration on plasma concentrations of raloxifene. Other Highly Protein-Bound Drugs --Raloxifene is more than 95% bound to plasma proteins. Other highly protein-bound drugs should not cause clinically relevant changes in EVISTA plasma concentrations. Furthermore, in the osteoporosis treatment trial, there were no clinically relevant effects of co-administration of other highly protein-bound drugs (e.g., gemfibrozil) on plasma concentrations of raloxifene. In vitro, raloxifene did not interact with the binding of phenytoin, tamoxifen, or warfarin (see above). Although not examined, EVISTA might affect the protein binding of other drugs and should be used with caution with certain other highly protein-bound drugs such as diazepam, diazoxide, and lidocaine. Carcinogenesis, Mutagenesis, and Impairment of FertilityCarcinogenesis --In a 21-month carcinogenicity study in mice, there was an increased incidence of ovarian tumors in female animals given 9 to 242 mg/kg, which included benign and malignant tumors of granulosa/theca cell origin and benign tumors of epithelial cell origin. Systemic exposure (AUC) of raloxifene in this group was 0.3 to 34 times that in postmenopausal women administered a 60-mg dose. There was also an increased incidence of testicular interstitial cell tumors and prostatic adenomas and adenocarcinomas in male mice given 41 or 210 mg/kg (4.7 or 24 times the AUC in humans), and prostatic leiomyoblastoma in male mice given 210 mg/kg. In a 2-year carcinogenicity study in rats, an increased incidence in ovarian tumors of granulosa/theca cell origin was observed in female rats given 279 mg/kg (approximately 400 times the AUC in humans). The female rodents in these studies were treated during their reproductive lives when their ovaries were functional and responsive to hormonal stimulation. Mutagenesis --Raloxifene HCl was not genotoxic in any of the following test systems: the Ames test for bacterial mutagenesis with and without metabolic activation, the unscheduled DNA synthesis assay in rat hepatocytes, the mouse lymphoma assay for mammalian cell mutation, the chromosomal aberration assay in Chinese hamster ovary cells, the in vivo sister chromatid exchange assay in Chinese hamsters, and the in vivo micronucleus test in mice. Impairment of Fertility --When male and female rats were given daily doses >/=5 mg/kg (>/=0.8 times the human dose based on surface area, mg/m 2 ) prior to and during mating, no pregnancies occurred. In male rats, daily doses up to 100 mg/kg (16 times the human dose based on surface area, mg/m 2 ) for at least 2 weeks did not affect sperm production or quality, or reproductive performance. In female rats, at doses of 0.1 to 10 mg/kg/day (0.02 to 1.6 times the human dose based on surface area, mg/m 2 ), raloxifene disrupted estrous cycles and inhibited ovulation. These effects of raloxifene were reversible. In another study in rats in which raloxifene was given during the preimplantation period at doses >/=0.1 mg/kg (>/=0.02 times the human dose based on surface area, mg/m 2 ), raloxifene delayed and disrupted embryo implantation resulting in prolonged gestation and reduced litter size. The reproductive and developmental effects observed in animals are consistent with the estrogen receptor activity of raloxifene. Pregnancy Category XEVISTA should not be used in women who are or may become pregnant ( see CONTRAINDICATIONS ). Nursing MothersEVISTA should not be used by lactating women ( see CONTRAINDICATIONS ). It is not known whether raloxifene is excreted in human milk. Pediatric UseEVISTA should not be used in pediatric patients. Geriatric UseIn the osteoporosis treatment trial of 7705 postmenopausal women, 4621 women were considered geriatric (greater than 65 years old). Of these, 845 women were greater than 75 years old. Safety and efficacy in older and younger postmenopausal women in the osteoporosis treatment trial appeared to be comparable.
ADVERSE REACTIONSAdverse Events in the Osteoporosis Treatment Clinical TrialThe safety of raloxifene in the treatment of osteoporosis was assessed in a large (7705 patients) multinational, placebo-controlled trial. Duration of treatment was 36 months and 5129 postmenopausal women were exposed to raloxifene (2557 received 60 mg/day and 2572 received 120 mg/day). The majority of adverse events occurring during the study were mild and generally did not require discontinuation of therapy. Therapy was discontinued due to an adverse event in 10.9% of EVISTA-treated women and 8.8% of placebo-treated women. Common adverse events considered to be related to EVISTA therapy were hot flashes and leg cramps. Hot flashes were most commonly reported during the first 6 months of treatment and were not different from placebo thereafter. Adverse Events in Placebo-Controlled Clinical Trials to Support the Osteoporosis Prevention IndicationThe safety of raloxifene has been assessed primarily in 12 Phase 2 and Phase 3 studies with placebo, estrogen, and estrogen-progestin replacement therapy (HRT) control groups. The duration of treatment ranged from 2 to 30 months and 2036 women were exposed to raloxifene (371 patients received 10 to 50 mg/day, 828 received 60 mg/day, and 837 received from 120 to 600 mg/day). The majority of adverse events occurring during clinical trials were mild and generally did not require discontinuation of therapy. Therapy was discontinued due to an adverse event in 11.4% of 581 EVISTA-treated women and 12.2% of 584 placebo-treated women. Common adverse events considered to be drug-related were hot flashes and leg cramps ( see Table 6). The first occurrence of hot flashes was most commonly reported during the first 6 months of treatment. Discontinuation rates due to hot flashes did not differ significantly between EVISTA and placebo groups (1.7% and 2.2%, respectively). Table 6 lists adverse events occurring in either the osteoporosis treatment or the prevention placebo-controlled clinical trial databases at a frequency >/=2.0% in either group and in more EVISTA-treated women than in placebo-treated women. Adverse events are shown without attribution of causality.
Comparison of EVISTA and Hormone Replacement Therapy Adverse EventsEVISTA was compared with estrogen-progestin replacement therapy (HRT) in three clinical trials for prevention of osteoporosis. Table 7 shows adverse events occurring more frequently in one treatment group and at an incidence >/=2.0% in any group. Adverse events are shown without attribution of causality.
Laboratory ChangesThe following changes in analyte concentrations are commonly observed during EVISTA therapy: increased apolipoprotein A1; and reduced serum total cholesterol, LDL cholesterol, fibrinogen, apolipoprotein B, and lipoprotein (a). EVISTA modestly increases hormone-binding globulin concentrations, including sex steroid-binding globulin, thyroxine-binding globulin, and corticosteroid-binding globulin with corresponding increases in measured total hormone concentrations. There is no evidence that these changes in hormone-binding globulin concentrations affect concentrations of the corresponding free hormones. There were small decreases in serum total calcium, inorganic phosphate, total protein, and albumin which were generally of lesser magnitude than decreases observed during ERT/HRT. Platelet count was also decreased slightly and was not different from ERT. Additional Safety InformationIncidences of estrogen-dependent carcinoma of the endometrium and breast are being evaluated across all completed and ongoing clinical trials involving 17,151 patients, of which at least 10,850 women have received at least one dose of raloxifene. These trials provided over 21,000 person-years of raloxifene exposure with a maximum exposure of 58 months. Endometrium --Compared to placebo, raloxifene did not increase the risk of endometrial cancer. Breast --Compared to placebo, raloxifene did not increase the risk of breast cancer ( see CLINICAL PHARMACOLOGY , Effects on the Breast ). Postintroduction ReportsAdverse events reported since market introduction include: very rarely--retinal vein occlusion.
OVERDOSAGEIncidents of overdose in humans have not been reported. In an 8-week study of 63 postmenopausal women, a dose of raloxifene HCl 600 mg/day was safely tolerated. No mortality was seen after a single oral dose in rats or mice at 5000 mg/kg (810 times the human dose for rats and 405 times the human dose for mice based on surface area, mg/m 2 ) or in monkeys at 1000 mg/kg (80 times the AUC in humans). There is no specific antidote for raloxifene.
DOSAGE AND ADMINISTRATIONThe recommended dosage is one 60-mg EVISTA tablet daily which may be administered any time of day without regard to meals.
HOW SUPPLIEDEVISTA 60-mg tablets are white, elliptical, and film coated. They are imprinted on one side with Lilly and the tablet code 4165 in edible blue ink. They are available as follows:
Store at controlled room temperature, 20° to 25°C (68° to 77°F) [ see USP]. The USP defines controlled room temperature as a temperature maintained thermostatically that encompasses the usual and customary working environment of 20° to 25°C (68° to 77°F); that results in a mean kinetic temperature calculated to be not more than 25°C; and that allows for excursions between 15° and 30°C (59° and 86°F) that are experienced in pharmacies, hospitals, and warehouses. Literature revised July 11, 2003 PV 3086 AMP Copyright © 1997, 2003, Eli Lilly and Company. All rights reserved.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 - To bookmark this page (add it to your favorites), please click the image to the left.
- To bookmark this page (add it to your favorites), please click the image to the left.