| DRUGS INDEX | MANUFACTURERS INDEX | ANATOMY | GEOGRAPHY | USA STATISTICS | CHINA STATISTICS | RELIGION | JOBS |
 |
||
Foradil Aerolizer (Schering) | ||
|
- Drugs index - Manufacturers - Feedback 
|
Prescribing Information DESCRIPTIONFORADIL® AEROLIZER® consists of a capsule dosage form containing a dry powder formulation of FORADIL (formoterol fumarate) intended for oral inhalation only with the AEROLIZER® Inhaler. Each clear, hard gelatin capsule contains a dry powder blend of 12 mcg of formoterol fumarate and 25 mg of lactose as a carrier. The active component of FORADIL is formoterol fumarate, a racemate. Formoterol fumarate is a selective beta 2 -adrenergic bronchodilator. Its chemical name is (±)-2-hydroxy-5-[(1RS)-1-hydroxy-2-[[(1RS)-2-(4-methoxyphenyl)-1-methylethyl]-amino]ethyl]formanilide fumarate dihydrate; its structural formula is
Formoterol fumarate has a molecular weight of 840.9, and its empirical formula is (C 19 H 24 N 2 O 4 ) 2 ·C 4 H 4 O 4 ·2H 2 O. Formoterol fumarate is a white to yellowish crystalline powder, which is freely soluble in glacial acetic acid, soluble in methanol, sparingly soluble in ethanol and isopropanol, slightly soluble in water, and practically insoluble in acetone, ethyl acetate, and diethyl ether. The AEROLIZER Inhaler is a plastic device used for inhaling FORADIL. The amount of drug delivered to the lung will depend on patient factors, such as inspiratory flow rate and inspiratory time. Under standardized in vitro testing at a fixed flow rate of 60 L/min for 2 seconds, the AEROLIZER Inhaler delivered 10 mcg of formoterol fumarate from the mouthpiece. Peak inspiratory flow rates (PIFR) achievable through the AEROLIZER Inhaler were evaluated in 33 adult and adolescent patients and 32 pediatric patients with mild-to-moderate asthma. Mean PIFR was 117.82 L/min (range 34-188 L/min) for adult and adolescent patients, and 99.66 L/min (range 43-187 L/min) for pediatric patients. Approximately ninety percent of each population studied generated a PIFR through the device exceeding 60 L/min. To use the delivery system, a FORADIL capsule is placed in the well of the AEROLIZER Inhaler, and the capsule is pierced by pressing and releasing the buttons on the side of the device. The formoterol fumarate formulation is dispersed into the air stream when the patient inhales rapidly and deeply through the mouthpiece.
CLINICAL PHARMACOLOGYMechanism of ActionFormoterol fumarate is a long-acting selective beta 2 -adrenergic receptor agonist (beta 2 -agonist). Inhaled formoterol fumarate acts locally in the lung as a bronchodilator. In vitro studies have shown that formoterol has more than 200-fold greater agonist activity at beta 2 -receptors than at beta 1 -receptors. Although beta 2 -receptors are the predominant adrenergic receptors in bronchial smooth muscle and beta 1 -receptors are the predominant receptors in the heart, there are also beta 2 -receptors in the human heart comprising 10%-50% of the total beta-adrenergic receptors. The precise function of these receptors has not been established, but they raise the possibility that even highly selective beta 2 -agonists may have cardiac effects. The pharmacologic effects of beta 2 -adrenoceptor agonist drugs, including formoterol, are at least in part attributable to stimulation of intracellular adenyl cyclase, the enzyme that catalyzes the conversion of adenosine triphosphate (ATP) to cyclic-3', 5'-adenosine monophosphate (cyclic AMP). Increased cyclic AMP levels cause relaxation of bronchial smooth muscle and inhibition of release of mediators of immediate hypersensitivity from cells, especially from mast cells. In vitro tests show that formoterol is an inhibitor of the release of mast cell mediators, such as histamine and leukotrienes, from the human lung. Formoterol also inhibits histamine-induced plasma albumin extravasation in anesthetized guinea pigs and inhibits allergen-induced eosinophil influx in dogs with airway hyper-responsiveness. The relevance of these in vitro and animal findings to humans is unknown. Animal PharmacologyStudies in laboratory animals (minipigs, rodents, and dogs) have demonstrated the occurrence of cardiac arrhythmias and sudden death (with histologic evidence of myocardial necrosis) when beta-agonists and methylxanthines are administered concurrently. The clinical significance of these findings is unknown. PharmacokineticsInformation on the pharmacokinetics of formoterol in plasma has been obtained in healthy subjects by oral inhalation of doses higher than the recommended range and in Chronic Obstructive Pulmonary Disease (COPD) patients after oral inhalation of doses at and above the therapeutic dose. Urinary excretion of unchanged formoterol was used as an indirect measure of systemic exposure. Plasma drug disposition data parallel urinary excretion, and the elimination half-lives calculated for urine and plasma are similar. AbsorptionFollowing inhalation of a single 120 mcg dose of formoterol fumarate by 12 healthy subjects, formoterol was rapidly absorbed into plasma, reaching a maximum drug concentration of 92 pg/mL within 5 minutes of dosing. In COPD patients treated for 12 weeks with formoterol fumarate 12 or 24 mcg b.i.d., the mean plasma concentrations of formoterol ranged between 4.0 and 8.8 pg/mL and 8.0 and 17.3 pg/mL, respectively, at 10 min, 2 h and 6 h post inhalation. Following inhalation of 12 to 96 mcg of formoterol fumarate by 10 healthy males, urinary excretion of both (R,R)- and (S,S)-enantiomers of formoterol increased proportionally to the dose. Thus, absorption of formoterol following inhalation appeared linear over the dose range studied. In a study in patients with asthma, when formoterol 12 or 24 mcg twice daily was given by oral inhalation for 4 weeks or 12 weeks, the accumulation index, based on the urinary excretion of unchanged formoterol ranged from 1.63 to 2.08 in comparison with the first dose. For COPD patients, when formoterol 12 or 24 mcg twice daily was given by oral inhalation for 12 weeks, the accumulation index, based on the urinary excretion of unchanged formoterol was 1.19-1.38. This suggests some accumulation of formoterol in plasma with multiple dosing. The excreted amounts of formoterol at steady-state were close to those predicted based on single-dose kinetics. As with many drug products for oral inhalation, it is likely that the majority of the inhaled formoterol fumarate delivered is swallowed and then absorbed from the gastrointestinal tract. DistributionThe binding of formoterol to human plasma proteins in vitro was 61%-64% at concentrations from 0.1 to 100 ng/mL. Binding to human serum albumin in vitro was 31%-38% over a range of 5 to 500 ng/mL. The concentrations of formoterol used to assess the plasma protein binding were higher than those achieved in plasma following inhalation of a single 120 mcg dose. MetabolismFormoterol is metabolized primarily by direct glucuronidation at either the phenolic or aliphatic hydroxyl group and O-demethylation followed by glucuronide conjugation at either phenolic hydroxyl groups. Minor pathways involve sulfate conjugation of formoterol and deformylation followed by sulfate conjugation. The most prominent pathway involves direct conjugation at the phenolic hydroxyl group. The second major pathway involves O-demethylation followed by conjugation at the phenolic 2'-hydroxyl group. Four cytochrome P450 isozymes (CYP2D6, CYP2C19, CYP2C9 and CYP2A6) are involved in the O-demethylation of formoterol. Formoterol did not inhibit CYP450 enzymes at therapeutically relevant concentrations. Some patients may be deficient in CYP2D6 or 2C19 or both. Whether a deficiency in one or both of these isozymes results in elevated systemic exposure to formoterol or systemic adverse effects has not been adequately explored. ExcretionFollowing oral administration of 80 mcg of radiolabeled formoterol fumarate to 2 healthy subjects, 59%-62% of the radioactivity was eliminated in the urine and 32%-34% in the feces over a period of 104 hours. Renal clearance of formoterol from blood in these subjects was about 150 mL/min. Following inhalation of a 12 mcg or 24 mcg dose by 16 patients with asthma, about 10% and 15%-18% of the total dose was excreted in the urine as unchanged formoterol and direct conjugates of formoterol, respectively. Following inhalation of 12 mcg or 24 mcg dose by 18 patients with COPD the corresponding values were 7% and 6-9% of the dose, respectively. Based on plasma concentrations measured following inhalation of a single 120 mcg dose by 12 healthy subjects, the mean terminal elimination half-life was determined to be 10 hours. From urinary excretion rates measured in these subjects, the mean terminal elimination half-lives for the (R,R)- and (S,S)-enantiomers were determined to be 13.9 and 12.3 hours, respectively. The (R,R)- and (S,S)-enantiomers represented about 40% and 60% of unchanged drug excreted in the urine, respectively, following single inhaled doses between 12 and 120 mcg in healthy volunteers and single and repeated doses of 12 and 24 mcg in patients with asthma. Thus, the relative proportion of the two enantiomers remained constant over the dose range studied and there was no evidence of relative accumulation of one enantiomer over the other after repeated dosing. Special PopulationsGender: After correction for body weight, formoterol pharmacokinetics did not differ significantly between males and females. Geriatric and Pediatric: The pharmacokinetics of formoterol have not been studied in the elderly population, and limited data are available in pediatric patients. In a study of children with asthma who were 5 to 12 years of age, when formoterol fumarate 12 or 24 mcg was given twice daily by oral inhalation for 12 weeks, the accumulation index ranged from 1.18 to 1.84 based on urinary excretion of unchanged formoterol. Hence, the accumulation in children did not exceed that in adults, where the accumulation index ranged from 1.63 to 2.08 (see above). Approximately 6% and 6.5% to 9% of the dose was recovered in the urine of the children as unchanged and conjugated formoterol, respectively. Hepatic/Renal Impairment: The pharmacokinetics of formoterol have not been studied in subjects with hepatic or renal impairment. PharmacodynamicsSystemic Safety and Pharmacokinetic/Pharmacodynamic RelationshipsThe major adverse effects of inhaled beta 2 -agonists occur as a result of excessive activation of the systemic beta-adrenergic receptors. The most common adverse effects in adults and adolescents include skeletal muscle tremor and cramps, insomnia, tachycardia, decreases in plasma potassium, and increases in plasma glucose. Pharmacokinetic/pharmacodynamic (PK/PD) relationships between heart rate, ECG parameters, and serum potassium levels and the urinary excretion of formoterol were evaluated in 10 healthy male volunteers (25 to 45 years of age) following inhalation of single doses containing 12, 24, 48, or 96 mcg of formoterol fumarate. There was a linear relationship between urinary formoterol excretion and decreases in serum potassium, increases in plasma glucose, and increases in heart rate. In a second study, PK/PD relationships between plasma formoterol levels and pulse rate, ECG parameters, and plasma potassium levels were evaluated in 12 healthy volunteers following inhalation of a single 120 mcg dose of formoterol fumarate (10 times the recommended clinical dose). Reductions of plasma potassium concentration were observed in all subjects. Maximum reductions from baseline ranged from 0.55 to 1.52 mmol/L with a median maximum reduction of 1.01 mmol/L. The formoterol plasma concentration was highly correlated with the reduction in plasma potassium concentration. Generally, the maximum effect on plasma potassium was noted 1 to 3 hours after peak formoterol plasma concentrations were achieved. A mean maximum increase of pulse rate of 26 bpm was observed 6 hours post dose. The maximum increase of mean corrected QT interval (QTc) was 25 msec when calculated using Bazett's correction and was 8 msec when calculated using Fredericia's correction. The QTc returned to baseline within 12-24 hours post-dose. Formoterol plasma concentrations were weakly correlated with pulse rate and increase of QTc duration. The effects on plasma potassium, pulse rate, and QTc interval are known pharmacological effects of this class of study drug and were not unexpected at the very high formoterol dose (120 mcg single dose, 10 times the recommended single dose) tested in this study. These effects were well-tolerated by the healthy volunteers. The electrocardiographic and cardiovascular effects of FORADIL AEROLIZER were compared with those of albuterol and placebo in two pivotal 12-week double-blind studies of patients with asthma. A subset of patients underwent continuous electrocardiographic monitoring during three 24-hour periods. No important differences in ventricular or supraventricular ectopy between treatment groups were observed. In these two studies, the total number of patients with asthma exposed to any dose of FORADIL AEROLIZER who had continuous electrocardiographic monitoring was about 200. Continuous electrocardiographic monitoring was not included in the clinical studies of FORADIL AEROLIZER that were performed in COPD patients. The electrocardiographic effects of FORADIL AEROLIZER were evaluated versus placebo in a 12-month pivotal double-blind study of patients with COPD. An analysis of ECG intervals was performed for patients who participated at study sites in the United States, including 46 patients treated with FORADIL AEROLIZER 12 mcg twice daily, and 50 patients treated with FORADIL AEROLIZER 24 mcg twice daily. ECGs were performed pre-dose, and at 5-15 minutes and 2 hours post-dose at study baseline and after 3, 6 and 12 months of treatment. The results showed that there was no clinically meaningful acute or chronic effect on ECG intervals, including QTc, resulting from treatment with FORADIL AEROLIZER. Tachyphylaxis/ToleranceIn a clinical study in 19 adult patients with mild asthma, the bronchoprotective effect of formoterol, as assessed by methacholine challenge, was studied following an initial dose of 24 mcg (twice the recommended dose) and after 2 weeks of 24 mcg twice daily. Tolerance to the bronchoprotective effects of formoterol was observed as evidenced by a diminished bronchoprotective effect on FEV 1 after 2 weeks of dosing, with loss of protection at the end of the 12 hour dosing period. Rebound bronchial hyper-responsiveness after cessation of chronic formoterol therapy has not been observed. In three large clinical trials in patients with asthma, while efficacy of formoterol versus placebo was maintained, a slightly reduced bronchodilatory response (as measured by 12-hour FEV 1 AUC) was observed within the formoterol arms over time, particularly with the 24 mcg twice daily dose (twice the daily recommended dose). A similarly reduced FEV 1 AUC over time was also noted in the albuterol treatment arms (180 mcg four times daily by metered-dose inhaler).
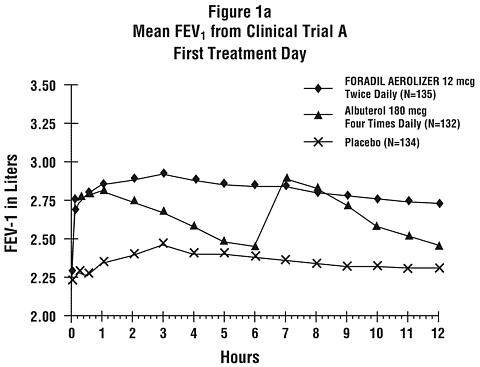
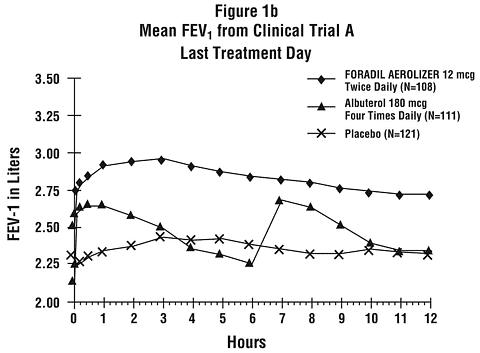
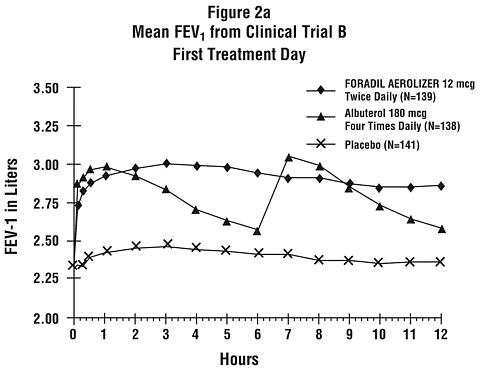
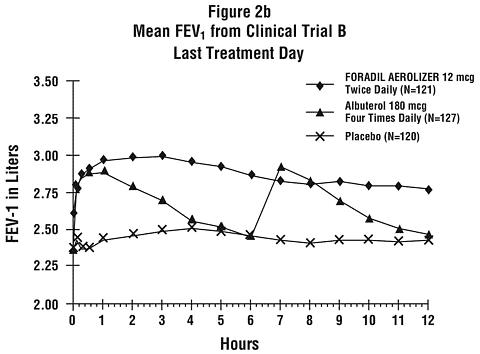
CLINICAL TRIALSAdolescent and Adult Asthma TrialsIn a placebo-controlled, single-dose clinical trial, the onset of bronchodilation (defined as a 15% or greater increase from baseline in FEV 1 ) was similar for FORADIL AEROLIZER and albuterol 180 mcg by metered-dose inhaler. In single-dose and multiple-dose clinical trials, the maximum improvement in FEV 1 for FORADIL AEROLIZER 12 mcg generally occurred within 1 to 3 hours, and an increase in FEV 1 above baseline was observed for 12 hours in most patients. FORADIL AEROLIZER was compared to albuterol 180 mcg four times daily by metered-dose inhaler, and placebo in a total of 1095 adult and adolescent patients 12 years of age and above with mild-to-moderate asthma (defined as FEV 1 40%-80% of the patient's predicted normal value) who participated in two pivotal, 12-week, multi-center, randomized, double-blind, parallel group studies. The results of both studies showed that FORADIL AEROLIZER 12 mcg twice daily resulted in significantly greater post-dose bronchodilation (as measured by serial FEV 1 for 12 hours post-dose) throughout the 12-week treatment period. Mean FEV 1 measurements from both studies are shown below for the first and last treatment days (see Figures 1 and 2).
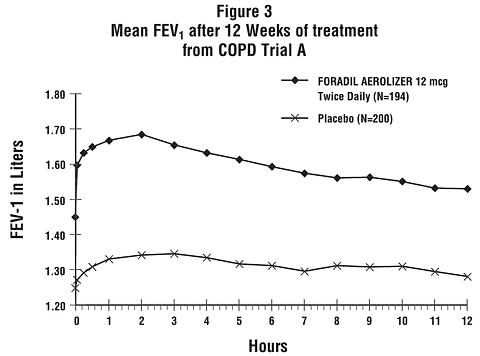
Compared with placebo and albuterol, patients treated with FORADIL AEROLIZER 12 mcg demonstrated improvement in many secondary efficacy endpoints, including improved combined and nocturnal asthma symptom scores, fewer nighttime awakenings, fewer nights in which patients used rescue medication, and higher morning and evening peak flow rates. Pediatric Asthma TrialA 12-month, multi-center, randomized, double-blind, parallel-group, study compared FORADIL AEROLIZER and placebo in a total of 518 children with asthma (ages 5-12 years) who required daily bronchodilators and anti-inflammatory treatment. Efficacy was evaluated on the first day of treatment, at Week 12, and at the end of treatment. FORADIL AEROLIZER 12 mcg twice daily demonstrated a greater 12-hour FEV 1 AUC compared to placebo on the first day of treatment, after twelve weeks of treatment, and after one year of treatment. Exercise-Induced Bronchospasm TrialsThe effect of FORADIL AEROLIZER on exercise-induced bronchospasm (defined as >20% fall in FEV 1 ) was examined in four randomized, single-dose, double-blind, crossover studies in a total of 77 patients 4 to 41 years of age with exercise-induced bronchospasm. Exercise challenge testing was conducted 15 minutes, and 4, 8, and 12 hours following administration of a single dose of study drug (FORADIL AEROLIZER 12 mcg, albuterol 180 mcg by metered-dose inhaler, or placebo) on separate test days. FORADIL AEROLIZER 12 mcg and albuterol 180 mcg were each superior to placebo for FEV 1 measurements obtained 15 minutes after study drug administration. FORADIL AEROLIZER 12 mcg maintained superiority over placebo at 4, 8, and 12 hours after administration. Most subjects were protected from exercise-induced bronchospasm for up to 12 hours following administration of FORADIL AEROLIZER; however, some were not. The efficacy of FORADIL AEROLIZER in the prevention of exercise-induced bronchospasm when dosed on a regular twice daily regimen has not been studied. Adult COPD TrialsIn multiple-dose clinical trials in patients with COPD, FORADIL AEROLIZER 12 mcg was shown to provide onset of significant bronchodilation (defined as 15% or greater increase from baseline in FEV 1 ) within 5 minutes of oral inhalation after the first dose. Bronchodilation was maintained for at least 12 hours. FORADIL AEROLIZER was studied in two pivotal, double-blind, placebo-controlled, randomized, multi-center, parallel-group trials in a total of 1634 adult patients (age range: 34-88 years; mean age: 63 years) with COPD who had a mean FEV 1 that was 46% of predicted. The diagnosis of COPD was based upon a prior clinical diagnosis of COPD, a smoking history (greater than 10 pack-years), age (at least 40 years), spirometry results (prebronchodilator baseline FEV 1 less than 70% of the predicted value, and at least 0.75 liters, with the FEV 1 /VC being less than 88% for men and less than 89% for women), and symptom score (greater than zero on at least four of the seven days prior to randomization). These studies included approximately equal numbers of patients with and without baseline bronchodilator reversibility, defined as a 15% or greater increase FEV 1 after inhalation of 200 mcg of albuterol sulfate. A total of 405 patients received FORADIL AEROLIZER 12 mcg, administered twice daily. Each trial compared FORADIL AEROLIZER 12 mcg twice daily and FORADIL AEROLIZER 24 mcg twice daily with placebo and an active control drug. The active control drug was ipratropium bromide in COPD Trial A, and slow-release theophylline in COPD Trial B (the theophylline arm in this study was open-label). The treatment period was 12 weeks in COPD Trial A, and 12 months in COPD Trial B. The results showed that FORADIL AEROLIZER 12 mcg twice daily resulted in significantly greater post-dose bronchodilation (as measured by serial FEV 1 for 12 hours post-dose; the primary efficacy analysis) compared to placebo when evaluated after 12 weeks of treatment in both trials, and after 12 months of treatment in the 12-month trial (COPD Trial B). Compared to FORADIL AEROLIZER 12 mcg twice daily, FORADIL AEROLIZER 24 mcg twice daily did not provide any additional benefit on a variety of endpoints including FEV 1 . Mean FEV 1 measurements after 12 weeks of treatment for one of the two major efficacy studies are shown in the figure below.
FORADIL AEROLIZER 12 mcg twice daily was statistically superior to placebo at all post-dose timepoints tested (from 5 minutes to 12 hours post-dose) throughout the 12-week (COPD Trial A) and 12-month (COPD Trial B) treatment periods. In both pivotal trials compared with placebo, patients treated with FORADIL AEROLIZER 12 mcg demonstrated improved morning pre-medication peak expiratory flow rates and took fewer puffs of rescue albuterol.
INDICATIONS AND USAGEFORADIL AEROLIZER is indicated for long-term, twice-daily (morning and evening) administration in the maintenance treatment of asthma and in the prevention of bronchospasm in adults and children 5 years of age and older with reversible obstructive airways disease, including patients with symptoms of nocturnal asthma, who require regular treatment with inhaled, short-acting, beta 2 -agonists. It is not indicated for patients whose asthma can be managed by occasional use of inhaled, short-acting, beta 2 -agonists. FORADIL AEROLIZER is also indicated for the acute prevention of exercise-induced bronchospasm (EIB) in adults and children 5 years of age and older, when administered on an occasional, as-needed basis. FORADIL AEROLIZER can be used to treat asthma concomitantly with short-acting beta 2 -agonists, inhaled or systemic corticosteroids, and theophylline therapy (see PRECAUTIONS , Drug Interactions ). A satisfactory clinical response to FORADIL AEROLIZER does not eliminate the need for continued treatment with an anti-inflammatory agent. FORADIL AEROLIZER is indicated for the long-term, twice daily (morning and evening) administration in the maintenance treatment of bronchoconstriction in patients with Chronic Obstructive Pulmonary Disease including chronic bronchitis and emphysema.
CONTRAINDICATIONSFORADIL (formoterol fumarate) is contraindicated in patients with a history of hypersensitivity to formoterol fumarate or to any components of this product.
WARNINGSIMPORTANT INFORMATION: FORADIL AEROLIZER SHOULD NOT BE INITIATED IN PATIENTS WITH SIGNIFICANTLY WORSENING OR ACUTELY DETERIORATING ASTHMA, WHICH MAY BE A LIFE-THREATENING CONDITION. The use of FORADIL AEROLIZER in this setting is inappropriate. FORADIL AEROLIZER IS NOT A SUBSTITUTE FOR INHALED OR ORAL CORTICOSTEROIDS. Corticosteroids should not be stopped or reduced at the time FORADIL AEROLIZER is initiated. (See PRECAUTIONS , Information for Patients and the accompanying Patient Instructions For Use.) When beginning treatment with FORADIL AEROLIZER, patients who have been taking inhaled, short-acting beta 2 -agonists on a regular basis (e.g., four times a day) should be instructed to discontinue the regular use of these drugs and use them only for symptomatic relief of acute asthma symptoms (see PRECAUTIONS , Information for Patients ). Paradoxical BronchospasmAs with other inhaled beta 2 -agonists, formoterol can produce paradoxical bronchospasm, that may be life-threatening. If paradoxical bronchospasm occurs, FORADIL AEROLIZER should be discontinued immediately and alternative therapy instituted. Deterioration of AsthmaAsthma may deteriorate acutely over a period of hours or chronically over several days or longer. If the usual dose of FORADIL AEROLIZER no longer controls the symptoms of bronchoconstriction, and the patient's inhaled, short-acting beta 2 -agonist becomes less effective or the patient needs more inhalation of short-acting beta 2 -agonist than usual, these may be markers of deterioration of asthma. In this setting, a re-evaluation of the patient and the asthma treatment regimen should be undertaken at once, giving special consideration to the possible need for anti-inflammatory treatment, e.g., corticosteroids. Increasing the daily dosage of FORADIL AEROLIZER beyond the recommended dose in this situation is not appropriate. FORADIL AEROLIZER should not be used more frequently than twice daily (morning and evening) at the recommended dose. Use of Anti-inflammatory AgentsThe use of beta 2 -agonists alone may not be adequate to control asthma in many patients. Early consideration should be given to adding anti-inflammatory agents, e.g., corticosteroids. There are no data demonstrating that FORADIL has any clinical anti-inflammatory effect and therefore it cannot be expected to take the place of corticosteroids. Patients who already require oral or inhaled corticosteroids for treatment of asthma should be continued on this type of treatment even if they feel better as a result of initiating or increasing the dose of FORADIL AEROLIZER. Any change in corticosteroid dosage, in particular a reduction, should be made ONLY after clinical evaluation (see PRECAUTIONS , Information for Patients ). Cardiovascular EffectsFormoterol fumarate, like other beta 2 -agonists, can produce a clinically significant cardiovascular effect in some patients as measured by increases in pulse rate, blood pressure, and/or symptoms. Although such effects are uncommon after administration of FORADIL AEROLIZER at recommended doses, if they occur, the drug may need to be discontinued. In addition, beta-agonists have been reported to produce ECG changes, such as flattening of the T wave, prolongation of the QTc interval, and ST segment depression. The clinical significance of these findings is unknown. Therefore, formoterol fumarate, like other sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension (see PRECAUTIONS , General ). Immediate Hypersensitivity ReactionsImmediate hypersensitivity reactions may occur after administration of FORADIL AEROLIZER, as demonstrated by cases of anaphylactic reactions, urticaria, angioedema, rash, and bronchospasm. Do Not Exceed Recommended DoseFatalities have been reported in association with excessive use of inhaled sympathomimetic drugs in patients with asthma. The exact cause of death is unknown, but cardiac arrest following an unexpected development of a severe acute asthmatic crisis and subsequent hypoxia is suspected.
PRECAUTIONSGeneralFORADIL AEROLIZER should not be used to treat acute symptoms of asthma. FORADIL AEROLIZER has not been studied in the relief of acute asthma symptoms and extra doses should not be used for that purpose. When prescribing FORADIL AEROLIZER, the physician should also provide the patient with an inhaled, short-acting beta 2 -agonist for treatment of symptoms that occur acutely, despite regular twice-daily (morning and evening) use of FORADIL AEROLIZER. Patients should also be cautioned that increasing inhaled beta 2 -agonist use is a signal of deteriorating asthma. (See Information for Patients and the accompanying Patient Instructions For Use.) Formoterol fumarate, like other sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension; in patients with convulsive disorders or thyrotoxicosis; and in patients who are unusually responsive to sympathomimetic amines. Clinically significant changes in systolic and/or diastolic blood pressure, pulse rate and electrocardiograms have been seen infrequently in individual patients in controlled clinical studies with formoterol. Doses of the related beta 2 -agonist albuterol, when administered intravenously, have been reported to aggravate preexisting diabetes mellitus and ketoacidosis. Beta-agonist medications may produce significant hypokalemia in some patients, possibly through intracellular shunting, which has the potential to produce adverse cardiovascular effects. The decrease in serum potassium is usually transient, not requiring supplementation. Clinically significant changes in blood glucose and/or serum potassium were infrequent during clinical studies with long-term administration of FORADIL AEROLIZER at the recommended dose. FORADIL® capsules should ONLY be used with the AEROLIZER® Inhaler and SHOULD NOT be taken orally. FORADIL® capsules should always be stored in the blister, and only removed IMMEDIATELY before use. Information for PatientsIt is important that patients understand how to use the AEROLIZER Inhaler appropriately and how it should be used in relation to other asthma medications they are taking (see the accompanying Patient Instructions For Use). The active ingredient of FORADIL (formoterol fumarate) is a long-acting, bronchodilator used for the treatment of asthma, including nocturnal asthma, and for the prevention of exercise-induced bronchospasm. FORADIL AEROLIZER provides bronchodilation for up to 12 hours. Patients should be advised not to increase the dose or frequency of FORADIL AEROLIZER without consulting the prescribing physician. Patients should be warned not to stop or reduce concomitant asthma therapy without medical advice. FORADIL AEROLIZER is not indicated to relieve acute asthma symptoms and extra doses should not be used for that purpose. Acute symptoms should be treated with an inhaled, short-acting, beta 2 -agonist (the health-care provider should prescribe the patient with such medication and instruct the patient in how it should be used). Patients should be instructed to seek medical attention if their symptoms worsen, if FORADIL AEROLIZER treatment becomes less effective, or if they need more inhalations of a short-acting beta 2 -agonist than usual. Patients should not inhale more than the contents of the prescribed number of capsules at any one time. The daily dosage of FORADIL AEROLIZER should not exceed one capsule twice daily (24 mcg total daily dose). When FORADIL AEROLIZER is used for the prevention of EIB, the contents of one capsule should be taken at least 15 minutes prior to exercise. Additional doses of FORADIL AEROLIZER should not be used for 12 hours. Prevention of EIB has not been studied in patients who are receiving chronic FORADIL AEROLIZER administration twice daily and these patients should not use additional FORADIL AEROLIZER for prevention of EIB. FORADIL AEROLIZER should not be used as a substitute for oral or inhaled corticosteroids. The dosage of these medications should not be changed and they should not be stopped without consulting the physician, even if the patient feels better after initiating treatment with FORADIL AEROLIZER. Patients should be informed that treatment with beta 2 -agonists may lead to adverse events which include palpitations, chest pain, rapid heart rate, tremor or nervousness. Patients should be informed never to use FORADIL AEROLIZER with a spacer and never to exhale into the device. Patients should avoid exposing the FORADIL capsules to moisture and should handle the capsules with dry hands. The AEROLIZER® Inhaler should never be washed and should be kept dry. The patient should always use the new AEROLIZER Inhaler that comes with each refill. Women should be advised to contact their physician if they become pregnant or if they are nursing. Patients should be told that in rare cases, the gelatin capsule might break into small pieces. These pieces should be retained by the screen built into the AEROLIZER Inhaler. However, it remains possible that rarely, tiny pieces of gelatin might reach the mouth or throat after inhalation. The capsule is less likely to shatter when pierced if: storage conditions are strictly followed, capsules are removed from the blister immediately before use, and the capsules are only pierced once. Drug InteractionsIf additional adrenergic drugs are to be administered by any route, they should be used with caution because the pharmacologically predictable sympathetic effects of formoterol may be potentiated. Concomitant treatment with xanthine derivatives, steroids, or diuretics may potentiate any hypokalemic effect of adrenergic agonists. The ECG changes and/or hypokalemia that may result from the administration of non-potassium sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by beta-agonists, especially when the recommended dose of the beta-agonist is exceeded. Although the clinical significance of these effects is not known, caution is advised in the co-administration of beta-agonist with non-potassium sparing diuretics. Formoterol, as with other beta 2 -agonists, should be administered with extreme caution to patients being treated with monamine oxidase inhibitors, tricyclic antidepressants, or drugs known to prolong the QTc interval because the action of adrenergic agonists on the cardiovascular system may be potentiated by these agents. Drugs that are known to prolong the QTc interval have an increased risk of ventricular arrhythmias. Beta-adrenergic receptor antagonists (beta-blockers) and formoterol may inhibit the effect of each other when administered concurrently. Beta-blockers not only block the therapeutic effects of beta-agonists, such as formoterol, but may produce severe bronchospasm in asthmatic patients. Therefore, patients with asthma should not normally be treated with beta-blockers. However, under certain circumstances, e.g., as prophylaxis after myocardial infarction, there may be no acceptable alternatives to the use of beta-blockers in patients with asthma. In this setting, cardioselective beta-blockers could be considered, although they should be administered with caution. Carcinogenesis, Mutagenesis, Impairment of FertilityThe carcinogenic potential of formoterol fumarate has been evaluated in 2-year drinking water and dietary studies in both rats and mice. In rats, the incidence of ovarian leiomyomas was increased at doses of 15 mg/kg and above in the drinking water study and at 20 mg/kg in the dietary study, but not at dietary doses up to 5 mg/kg (AUC exposure approximately 450 times human exposure at the maximum recommended daily inhalation dose). In the dietary study, the incidence of benign ovarian thecacell tumors was increased at doses of 0.5 mg/kg and above (AUC exposure at the low dose of 0.5 mg/kg was approximately 45 times human exposure at the maximum recommended daily inhalation dose). This finding was not observed in the drinking water study, nor was it seen in mice (see below). In mice, the incidence of adrenal subcapsular adenomas and carcinomas was increased in males at doses of 69 mg/kg and above in the drinking water study, but not at doses up to 50 mg/kg (AUC exposure approximately 590 times human exposure at the maximum recommended daily inhalation dose) in the dietary study. The incidence of hepatocarcinomas was increased in the dietary study at doses of 20 and 50 mg/kg in females and 50 mg/kg in males, but not at doses up to 5 mg/kg in either males or females (AUC exposure approximately 60 times human exposure at the maximum recommended daily inhalation dose). Also in the dietary study, the incidence of uterine leiomyomas and leiomyosarcomas was increased at doses of 2 mg/kg and above (AUC exposure at the low dose of 2 mg/kg was approximately 25 times human exposure at the maximum recommended daily inhalation dose). Increases in leiomyomas of the rodent female genital tract have been similarly demonstrated with other beta-agonist drugs. Formoterol fumarate was not mutagenic or clastogenic in the following tests: mutagenicity tests in bacterial and mammalian cells, chromosomal analyses in mammalian cells, unscheduled DNA synthesis repair tests in rat hepatocytes and human fibroblasts, transformation assay in mammalian fibroblasts and micronucleus tests in mice and rats. Reproduction studies in rats revealed no impairment of fertility at oral doses up to 3 mg/kg (approximately 1000 times the maximum recommended daily inhalation dose in humans on a mg/m 2 basis). Pregnancy, Teratogenic Effects, Pregnancy Category CFormoterol fumarate has been shown to cause stillbirth and neonatal mortality at oral doses of 6 mg/kg (approximately 2000 times the maximum recommended daily inhalation dose in humans on a mg/m 2 basis) and above in rats receiving the drug during the late stage of pregnancy. These effects, however, were not produced at a dose of 0.2 mg/kg (approximately 70 times the maximum recommended daily inhalation dose in humans on a mg/m 2 basis). When given to rats throughout organogenesis, oral doses of 0.2 mg/kg and above delayed ossification of the fetus, and doses of 6 mg/kg and above decreased fetal weight. Formoterol fumarate did not cause malformations in rats or rabbits following oral administration. Because there are no adequate and well-controlled studies in pregnant women, FORADIL AEROLIZER should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Use in Labor and DeliveryFormoterol fumarate has been shown to cause stillbirth and neonatal mortality at oral doses of 6 mg/kg (approximately 2000 times the maximum recommended daily inhalation dose in humans on a mg/m 2 basis) and above in rats receiving the drug for several days at the end of pregnancy. These effects were not produced at a dose of 0.2 mg/kg (approximately 70 times the maximum recommended daily inhalation dose in humans on a mg/m 2 basis). There are no adequate and well-controlled human studies that have investigated the effects of FORADIL AEROLIZER during labor and delivery. Because beta-agonists may potentially interfere with uterine contractility, FORADIL AEROLIZER should be used during labor only if the potential benefit justifies the potential risk. Nursing MothersIn reproductive studies in rats, formoterol was excreted in the milk. It is not known whether formoterol is excreted in human milk, but because many drugs are excreted in human milk, caution should be exercised if FORADIL AEROLIZER is administered to nursing women. There are no well-controlled human studies of the use of FORADIL AEROLIZER in nursing mothers. Pediatric UseAsthmaA total of 776 children 5 years of age and older with asthma were studied in three multiple-dose controlled clinical trials. Of the 512 children who received formoterol, 508 were 5-12 years of age, and approximately one third were 5-8 years of age. Exercise-Induced BronchospasmA total of 25 pediatric patients, 4-11 years of age, were studied in two well-controlled single-dose clinical trials. The safety and effectiveness of FORADIL AEROLIZER in pediatric patients below 5 years of age has not been established. (See CLINICAL TRIALS , Pediatric Asthma Trial , and ADVERSE REACTIONS , Experience in Pediatric, Adolescent and Adult Patients .) Geriatric UseOf the total number of patients who received FORADIL AEROLIZER in adolescent and adult chronic dosing asthma clinical trials, 318 were 65 years of age or older and 39 were 75 years of age and older. Of the 811 patients who received FORADIL AEROLIZER in two pivotal multiple-dose controlled clinical studies in patients with COPD, 395 (48.7%) were 65 years of age or older while 62 (7.6%) were 75 years of age or older. No overall differences in safety or effectiveness were observed between these subjects and younger subjects. A slightly higher frequency of chest infection was reported in the 39 asthma patients 75 years of age and older, although a causal relationship with FORADIL has not been established. Other reported clinical experience has not identified differences in responses between the elderly and younger adult patients, but greater sensitivity of some older individuals cannot be ruled out. (See PRECAUTIONS , Drug Interactions .)
ADVERSE REACTIONSAdverse reactions to FORADIL are similar in nature to other selective beta 2 -adrenoceptor agonists; e.g., angina, hypertension or hypotension, tachycardia, arrhythmias, nervousness, headache, tremor, dry mouth, palpitation, muscle cramps, nausea, dizziness, fatigue, malaise, hypokalemia, hyperglycemia, metabolic acidosis and insomnia. Experience in Pediatric, Adolescent and Adult Patients with AsthmaOf the 5,824 patients in multiple-dose controlled clinical trials, 1,985 were treated with FORADIL AEROLIZER at the recommended dose of 12 mcg twice daily. The following table shows adverse events where the frequency was greater than or equal to 1% in the FORADIL twice daily group and where the rates in the FORADIL group exceeded placebo. Three adverse events showed dose ordering among tested doses of 6, 12 and 24 mcg administered twice daily; tremor, dizziness and dysphonia.
Experience in Children with AsthmaThe safety of FORADIL AEROLIZER compared to placebo was investigated in one large, multicenter, randomized, double-blind clinical trial in 518 children with asthma (ages 5-12 years) in need of daily bronchodilators and anti-inflammatory treatment. The numbers and percent of patients who reported adverse events were comparable in the 12 mcg twice daily and placebo groups. In general, the pattern of the adverse events observed in children differed from the usual pattern seen in adults. The adverse events that were more frequent in the formoterol group than in the placebo group reflected infection/inflammation (viral infection, rhinitis, tonsillitis, gastroenteritis) or abdominal complaints (abdominal pain, nausea, dyspepsia). Experience in Adult Patients with COPDOf the 1634 patients in two pivotal multiple-dose Chronic Obstructive Pulmonary Disease (COPD) controlled trials, 405 were treated with FORADIL AEROLIZER 12 mcg twice daily. The numbers and percent of patients who reported adverse events were comparable in the 12 mcg twice daily and placebo groups. Adverse events (AE's) experienced were similar to those seen in asthmatic patients, but with a higher incidence of COPD-related AE's in both placebo and formoterol treated patients. The following table shows adverse events where the frequency was greater than or equal to 1% in the FORADIL AEROLIZER group and where the rates in the FORADIL AEROLIZER group exceeded placebo. The two clinical trials included doses of 12 mcg and 24 mcg, administered twice daily. Seven adverse events showed dose ordering among tested doses of 12 and 24 mcg administered twice daily; pharyngitis, fever, muscle cramps, increased sputum, dysphonia, myalgia, and tremor.
Overall, the frequency of all cardiovascular adverse events in the two pivotal studies was low and comparable to placebo (6.4% for FORADIL AEROLIZER 12 mcg twice daily, and 6.0% for placebo). There were no frequently-occurring specific cardiovascular adverse events for FORADIL AEROLIZER (frequency greater than or equal to 1% and greater than placebo). Post Marketing ExperienceIn extensive worldwide marketing experience with FORADIL, serious exacerbations of asthma, including some that have been fatal, have been reported. While most of these cases have been in patients with severe or acutely deteriorating asthma (see WARNINGS ), a few have occurred in patients with less severe asthma. The contribution of FORADIL to these cases could not be determined. Rare reports of anaphylactic reactions, including severe hypotension and angioedema, have also been received in association with the use of formoterol fumarate inhalation powder.
DRUG ABUSE AND DEPENDENCEThere was no evidence in clinical trials of drug dependence with the use of FORADIL.
OVERDOSAGEThe expected signs and symptoms with overdosage of FORADIL AEROLIZER are those of excessive beta-adrenergic stimulation and/or occurrence or exaggeration of any of the signs and symptoms listed under ADVERSE REACTIONS , e.g., angina, hypertension or hypotension, tachycardia, with rates up to 200 beats/min., arrhythmias, nervousness, headache, tremor, seizures, muscle cramps, dry mouth, palpitation, nausea, dizziness, fatigue, malaise, hypokalemia, hyperglycemia, and insomnia. Metabolic acidosis may also occur. As with all inhaled sympathomimetic medications, cardiac arrest and even death may be associated with an overdose of FORADIL AEROLIZER. Treatment of overdosage consists of discontinuation of FORADIL AEROLIZER together with institution of appropriate symptomatic and/or supportive therapy. The judicious use of a cardioselective beta-receptor blocker may be considered, bearing in mind that such medication can produce bronchospasm. There is insufficient evidence to determine if dialysis is beneficial for overdosage of FORADIL AEROLIZER. Cardiac monitoring is recommended in cases of overdosage. The minimum acute lethal inhalation dose of formoterol fumarate in rats is 156 mg/kg (approximately 53,000 and 25,000 times the maximum recommended daily inhalation dose in adults and children, respectively, on a mg/m 2 basis). The median lethal oral doses in Chinese hamsters, rats, and mice provide even higher multiples of the maximum recommended daily inhalation dose in humans.
DOSAGE AND ADMINISTRATIONFORADIL capsules should be administered only by the oral inhalation route (see the accompanying Patient Instructions for Use) and only using the AEROLIZER Inhaler. FORADIL capsules should not be ingested (i.e., swallowed) orally. FORADIL capsules should always be stored in the blister, and only removed IMMEDIATELY BEFORE USE. For Maintenance Treatment of AsthmaFor adults and children 5 years of age and older, the usual dosage is the inhalation of the contents of one 12-mcg FORADIL capsule every 12 hours using the AEROLIZER® Inhaler. The patient must not exhale into the device. The total daily dose of FORADIL should not exceed one capsule twice daily (24 mcg total daily dose). More frequent administration or administration of a larger number of inhalations is not recommended. If symptoms arise between doses, an inhaled short-acting beta 2 -agonist should be taken for immediate relief. If a previously effective dosage regimen fails to provide the usual response, medical advice should be sought immediately as this is often a sign of destabilization of asthma. Under these circumstances, the therapeutic regimen should be re-evaluated and additional therapeutic options, such as inhaled or systemic corticosteroids, should be considered. For Prevention of Exercise-Induced Bronchospasm (EIB)For adults and children 5 years of age or older, the usual dosage is the inhalation of the contents of one 12-mcg FORADIL capsule at least 15 minutes before exercise administered on an occasional as-needed basis. When used intermittently as needed for prevention, protection may last up to 12 hours. Additional doses of FORADIL AEROLIZER should not be used for 12 hours after the administration of this drug. Regular, twice-daily dosing has not been studied in preventing EIB. Patients who are receiving FORADIL AEROLIZER twice daily for maintenance treatment of their asthma should not use additional doses for prevention of EIB and may require a short-acting bronchodilator. For Maintenance Treatment of Chronic Obstructive Pulmonary Disease (COPD)The usual dosage is the inhalation of the contents of one 12 mcg FORADIL capsule every 12 hours using the AEROLIZER® inhaler. A total daily dose of greater than 24 mcg is not recommended. If a previously effective dosage regimen fails to provide the usual response, medical advice should be sought immediately as this is often a sign of destabilization of COPD. Under these circumstances, the therapeutic regimen should be re-evaluated and additional therapeutic options should be considered.
HOW SUPPLIEDFORADIL® AEROLIZER® contains: aluminum blister-packaged 12-mcg FORADIL (formoterol fumarate) clear gelatin capsules with "CG" printed on one end and "FXF" printed on the opposite end; one AEROLIZER® Inhaler; and Patient Instructions for Use
FORADIL® capsules should be used with the AEROLIZER® Inhaler only. The AEROLIZER® Inhaler should not be used with any other capsules. Prior to dispensing: Store in a refrigerator, 2°C-8°C (36°F-46°F) After dispensing to patient: Store at 20°C to 25°C (68°F to 77°F) [see USP Controlled Room Temperature]. Protect from heat and moisture. CAPSULES SHOULD ALWAYS BE STORED IN THE BLISTER AND ONLY REMOVED FROM THE BLISTER IMMEDIATELY BEFORE USE. Always discard the FORADIL® capsules and AEROLIZER® Inhaler by the "Use by" date and always use the new AEROLIZER Inhaler provided with each new prescription. Keep out of the reach of children.
Manufactured by: Novartis Pharma AG, Basle, Switzerland for Schering Corporation, Kenilworth, NJ 07033 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 - To bookmark this page (add it to your favorites), please click the image to the left.
- To bookmark this page (add it to your favorites), please click the image to the left.