| DRUGS INDEX | MANUFACTURERS INDEX | ANATOMY | GEOGRAPHY | USA STATISTICS | CHINA STATISTICS | RELIGION | JOBS |
 |
||
Tequin Injection, Tequin Tablets (Bristol-Myers Squibb) | ||
|
- Drugs index - Manufacturers - Feedback 
|
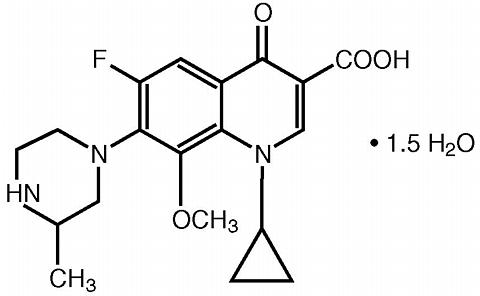
TEQUIN ® is available as TEQUIN (gatifloxacin) Tablets for oral administration and TEQUIN (gatifloxacin) Injection and TEQUIN (gatifloxacin in 5% dextrose) Injection for intravenous administration. To reduce the development of drug-resistant bacteria and maintain the effectiveness of TEQUIN and other antibacterial drugs, TEQUIN should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria. DESCRIPTIONTEQUIN contains gatifloxacin, a synthetic broad-spectrum 8-methoxyfluoroquinolone antibacterial agent for oral or intravenous administration. Chemically, gatifloxacin is (±) -1-cyclopropyl-6-fluoro-1, 4-dihydro-8-methoxy-7-(3-methyl-1-piperazinyl)-4-oxo-3-quinolinecarboxylic acid sesquihydrate. The chemical structure is:
Its empirical formula is C 19 H 22 FN 3 O 4 ·1.5 H 2 O and its molecular weight is 402.42. Gatifloxacin is a sesquihydrate crystalline powder and is white to pale yellow in color. It exists as a racemate, with no net optical rotation. The solubility of the compound is pH dependent. The maximum aqueous solubility (40-60 mg/mL) occurs at a pH range of 2 to 5. TEQUIN Tablets TEQUIN Tablets are available as 200-mg and 400-mg white, film-coated tablets and contain the following inactive ingredients: hypromellose, magnesium stearate, methylcellulose, microcrystalline cellulose, polyethylene glycol, polysorbate 80, simethicone, sodium starch glycolate, sorbic acid, and titanium dioxide. TEQUIN Injection for Intravenous Administration TEQUIN Injection is available in 40-mL (400-mg) single-use vials as a sterile, preservative-free aqueous solution of gatifloxacin with pH ranging from 3.5 to 5.5. TEQUIN (gatifloxacin in 5% dextrose) Injection is also available in ready-to-use 100-mL (200-mg) and 200-mL (400-mg) flexible bags as a sterile, preservative-free aqueous solution of gatifloxacin with pH ranging from 3.5 to 5.5. The appearance of the intravenous solution may range from light yellow to greenish-yellow in color. The color does not affect nor is it indicative of product stability. The intravenous formulation contains dextrose, anhydrous, USP or dextrose, monohydrate, USP and Water for Injection, USP, and may contain hydrochloric acid and/or sodium hydroxide for pH adjustment.
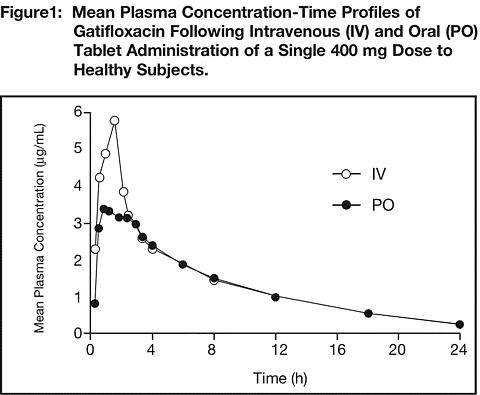
CLINICAL PHARMACOLOGYGatifloxacin is administered as a racemate, with the disposition and antibacterial activity of the R- and S-enantiomers virtually identical. AbsorptionGatifloxacin is well absorbed from the gastrointestinal tract after oral administration and can be given without regard to food. The absolute bioavailability of gatifloxacin tablets is 96%. Peak plasma concentrations of gatifloxacin usually occur 1-2 hours after oral dosing under fasted conditions. The oral and intravenous routes of administration for TEQUIN can be considered interchangeable, since the pharmacokinetics of gatifloxacin after 1-hour intravenous administration are similar to those observed for orally administered gatifloxacin when equal doses are administered (Figure 1) (see DOSAGE AND ADMINISTRATION ). TEQUIN Tablets and Oral Suspension can be considered interchangeable since they are bioequivalent.
PharmacokineticsThe mean (SD) pharmacokinetic parameters of gatifloxacin following oral administration to healthy subjects with bacterial infections and subjects with renal insufficiency are listed in Table 1. The mean (SD) pharmacokinetic parameters of gatifloxacin following intravenous administration to healthy subjects are listed in Table 2.
Gatifloxacin pharmacokinetics are linear and time-independent at doses ranging from 200 to 800 mg administered over a period of up to 14 days. Steady-state concentrations are achieved by the third daily oral or intravenous dose of gatifloxacin. The mean steady-state peak and trough plasma concentrations attained following a dosing regimen of 400 mg once daily are approximately 4.2 mcg/mL and 0.4 mcg/mL, respectively, for oral administration and 4.6 mcg/mL and 0.4 mcg/mL, respectively, for intravenous administration. The tablets and oral suspension are bioequivalent and are anticipated to result in similar steady-state exposures. DistributionSerum protein binding of gatifloxacin is approximately 20% in volunteers and is concentration independent. Consistent with the low protein binding, concentrations of gatifloxacin in saliva were approximately equal to those in plasma (mean [range] saliva:plasma ratio was 0.88 [0.46-1.57]). The mean volume of distribution of gatifloxacin at steady-state (Vd ss ) ranged from 1.5 to 2.0 L/kg. Gatifloxacin is widely distributed throughout the body into many body tissues and fluids. Rapid distribution of gatifloxacin into tissues results in higher gatifloxacin concentrations in most target tissues than in serum (Table 3).
MetabolismGatifloxacin undergoes limited biotransformation in humans with less than 1% of the dose excreted in the urine as ethylenediamine and methylethylenediamine metabolites. In vitro studies with cytochrome P450 isoenzymes (CYP) indicate that gatifloxacin does not inhibit CYP3A4, CYP2D6, CYP2C9, CYP2C19, or CYP1A2, suggesting that gatifloxacin is unlikely to alter the pharmacokinetics of drugs metabolized by these enzymes (eg, midazolam, cyclosporine, warfarin, theophylline). In vivo studies in animals and humans indicate that gatifloxacin is not an enzyme inducer; therefore, gatifloxacin is unlikely to alter the metabolic elimination of itself or other coadministered drugs. ExcretionGatifloxacin is excreted as unchanged drug primarily by the kidney. More than 70% of an administered TEQUIN (gatifloxacin) dose was recovered as unchanged drug in the urine within 48 hours following oral and intravenous administration, and 5% was recovered in the feces. Less than 1% of the dose is recovered in the urine as two metabolites. Crystals of gatifloxacin have not been observed in the urine of normal, healthy human subjects following administration of intravenous or oral doses up to 800 mg. The mean elimination half-life of gatifloxacin ranges from 7 to 14 hours and is independent of dose and route of administration. Renal clearance is independent of dose with mean value ranging from 124 to 161 mL/min. The magnitude of this value, coupled with the significant decrease in the elimination of gatifloxacin seen with concomitant probenecid administration, indicates that gatifloxacin undergoes both glomerular filtration and tubular secretion. Gatifloxacin may also undergo minimal biliary and/or intestinal elimination, since 5% of dose was recovered in the feces as unchanged drug. This finding is supported by the 5-fold higher concentration of gatifloxacin in the bile compared to the plasma (mean bile:plasma ratio [range] 5.34 [0.33-14.0]). Special PopulationsPatients with Bacterial Infections The pharmacokinetics of gatifloxacin were similar between healthy volunteers and patients with infection, when underlying renal function was taken into account (see Table 1). Geriatric Following a single oral 400-mg dose of gatifloxacin in young (18-40 years) and elderly (>/=65 years) male and female subjects, there were only modest differences in the pharmacokinetics of gatifloxacin noted in female subjects; elderly females had a 21% increase in C max and a 32% increase in AUC (0-(infinity)) compared to young females. These differences were mainly due to decreasing renal function with increasing age and are not thought to be clinically important. No dosage adjustment based on age alone is necessary for elderly subjects when administering TEQUIN. Pediatric The pharmacokinetics of gatifloxacin in pediatric populations (<18 years of age) have not been established. Gender Following a single oral 400-mg dose of gatifloxacin in male and female subjects, there were only modest differences in the pharmacokinetics of gatifloxacin, mainly confined to elderly subjects. Elderly females had a 21% increase in C max and a 33% increase in AUC (0-(infinity)) compared to elderly males. Both results were accounted for by gender-related differences in body weight and are not thought to be clinically important. Dosage adjustment of TEQUIN is not necessary based on gender. Chronic Hepatic Disease Following a single oral 400-mg dose of gatifloxacin in healthy subjects and in subjects with moderate hepatic impairment (Child-Pugh B classification of cirrhosis), C max and AUC (0-(infinity)) values for gatifloxacin were modestly higher (32% and 23% respectively). Due to the concentration-dependent antimicrobial activity associated with quinolones, the modestly higher C max values in the subjects with moderate hepatic impairment are not expected to negatively impact the outcome of TEQUIN therapy in this population. Dosage adjustment of TEQUIN is not necessary in patients with moderate hepatic impairment. The effect of severe hepatic impairment on the pharmacokinetics of TEQUIN is unknown. Renal Insufficiency Following administration of a single oral 400-mg dose of gatifloxacin to subjects with varying degrees of renal impairment, apparent total clearance of gatifloxacin (Cl/F) was reduced and systemic exposure (AUC) was increased commensurate with the decrease in renal function (see Table 1). Total gatifloxacin clearance was reduced 57% in moderate renal insufficiency (Cl cr 30-49 mL/min) and 77% in severe renal insufficiency (Cl cr <30 mL/min). Systemic exposure to gatifloxacin was approximately 2 times higher in moderate renal insufficiency and approximately 4 times higher in severe renal insufficiency, compared to subjects with normal renal function. Mean C max values were modestly increased. A reduced dosage of TEQUIN is recommended in patients with creatinine clearance <40 mL/min, including patients requiring hemodialysis or continuous ambulatory peritoneal dialysis (CAPD) [see PRECAUTIONS : General and DOSAGE AND ADMINISTRATION : Impaired Renal Function ). Diabetes Mellitus The pharmacokinetics of gatifloxacin in patients with type 2 diabetes (non-insulin-dependent diabetes mellitus), following TEQUIN 400 mg orally for 10 days, were comparable to those in healthy subjects. Glucose HomeostasisDisturbances of blood glucose, including symptomatic hyper- and hypoglycemia, have been reported with TEQUIN, usually in diabetic patients. Therefore, careful monitoring of blood glucose is recommended when TEQUIN is administered to patients with diabetes (see WARNINGS , PRECAUTIONS : Information for Patients , and Drug Interactions , and ANIMAL PHARMACOLOGY ). In a postmarketing study conducted in non-infected patients (n=70) with type 2 diabetes mellitus controlled primarily with either the combination of glyburide and metformin or metformin alone, daily administration of gatifloxacin 400 mg orally for 14 days was associated with initial hypoglycemia followed by hyperglycemia. Upon initiation of gatifloxacin dosing (i.e., first 2 days of treatment), there were increases in serum insulin concentrations and resulting decreases in serum glucose, as compared to baseline glucose values, despite ingestion of dietary restricted meals. In some patients, the reductions in glucose produced signs and symptoms of hypoglycemia (asthenia, sweating, dizziness) and necessitated administration of additional food. With continued gatifloxacin dosing (i.e., from the third day of treatment and throughout the dosing period) fasting serum glucose concentrations were increased compared to baseline. The serum glucose concentrations returned to baseline in most of these uninfected patients by 28 days after the cessation of gatifloxacin treatment. Single doses of insulin were administered to three patients in this study to correct the hyperglycemia during continued gatifloxacin administration. In two premarketing studies, no clinically significant changes in glucose tolerance (via measurement of oral glucose challenge) and glucose homeostasis (via measurement of fasting serum glucose, serum insulin, and c-peptide) were observed following single or multiple intravenous infusion doses of 200 to 800 mg TEQUIN in healthy volunteers (n=30), or 400-mg oral doses of TEQUIN for 10 days in patients (n=16) with type 2 (non-insulin-dependent) diabetes mellitus controlled on diet and exercise. Compared to placebo, transient modest increases in serum insulin of approximately 20-40% and decreases in glucose concentrations of approximately 30% were noted with the first dose of intravenous or oral gatifloxacin. In another premarketing study, following administration of single oral 400-mg doses of TEQUIN for 10 days in patients (n=16) with type 2 diabetes mellitus controlled with glyburide, decreases in serum insulin concentrations of approximately 30-40%, as compared to placebo, were noted following oral glucose challenge; however, these decreases were not accompanied by statistically significant changes in serum glucose levels. In this study, modest increases in fasting glucose (average increases of 40 mg/dL) were also noted by day 4 of continued gatifloxacin administration, although these changes did not reach statistical significance. Photosensitivity PotentialIn a study of the skin response to ultraviolet and visible radiation conducted in 48 healthy, male Caucasian volunteers (12 per group), the minimum erythematous dose was measured for ciprofloxacin (500 mg BID), lomefloxacin (400 mg QD), gatifloxacin (400 mg QD), and placebo before and after drug administration for 7 days. In this study, gatifloxacin was comparable to placebo at all wavelengths tested and had a lower potential for producing delayed photosensitivity skin reactions than ciprofloxacin or lomefloxacin. ElectrocardiogramIn premarketing studies of volunteer subjects with pre- and post-dose ECGs obtained in 55 male volunteers receiving oral or IV TEQUIN doses of 200 to 800 mg, the mean change in the post-dose QTc interval was <10 msec and there were no subjects with prolonged post-dose QTc intervals of >450 msec. In a postmarketing study of 34 healthy male and female volunteers receiving single oral doses of TEQUIN 400, 800, and 1200 mg and placebo, an association between increases in post-dose QTc interval changes from baseline and increases in gatifloxacin plasma concentrations were observed. At the therapeutic dose of 400 mg, the mean change in the post-dose QTc interval from baseline was <10 msec. There were no subjects with prolonged post-dose QTc intervals of >450 msec for males and >470 msec for females. In a postmarketing clinical trial of 262 patients with respiratory tract infections receiving repeated 400-mg oral doses of TEQUIN who were studied with pre- and post-dose ECGs, the mean change in the post-dose QTc interval was <10 msec following the first 400-mg dose. In another postmarketing study of patients, with an acute coronary syndrome occurring within 4 weeks prior to TEQUIN (gatifloxacin) administration, pre- and post-dose ECGs were obtained in patients who were administered TEQUIN 400 mg orally after single (n=372) and repeated (steady state; n=36) dosing. The mean changes in the post-dose QTc interval in these patients were <10 msec after both single and repeated dosing. There is limited information available on the potential for a pharmacodynamic interaction in humans between gatifloxacin and drugs that prolong the QTc interval of an electrocardiogram such as Class IA and Class III antiarrhythmics, cisapride, erythromycin, antipsychotics, and tricyclic antidepressants (see WARNINGS and PRECAUTIONS : Information for Patients ). SpirometryNo clinically significant changes in spirometry were observed following single or multiple 200-mg, 400-mg, 600-mg, and 800-mg intravenous infusion doses of TEQUIN in healthy volunteers. Drug-Drug InteractionsSystemic exposure to TEQUIN is increased following concomitant administration of TEQUIN and probenecid, and is reduced by concomitant administration of TEQUIN and ferrous sulfate or antacids containing aluminum or magnesium salts. TEQUIN can be administered 4 hours before the administration of dietary supplements containing zinc, magnesium, or iron (such as multivitamins).
Minor pharmacokinetic interactions occur following concomitant administration of gatifloxacin and digoxin; a priori dosage adjustments of either drug are not warranted.
No significant pharmacokinetic interactions occur when cimetidine, omeprazole, midazolam, theophylline, warfarin, or glyburide is administered concomitantly with TEQUIN. These results and the data from in vitro studies suggest that gatifloxacin is unlikely to significantly alter the metabolic clearance of drugs metabolized by CYP3A, CYP1A2, CYP2C9, CYP2C19, and CYP2D6 isoenzymes.
MicrobiologyGatifloxacin is an 8-methoxyfluoroquinolone with in vitro activity against a wide range of gram-negative and gram-positive microorganisms. The antibacterial action of gatifloxacin results from inhibition of DNA gyrase and topoisomerase IV. DNA gyrase is an essential enzyme that is involved in the replication, transcription, and repair of bacterial DNA. Topoisomerase IV is an enzyme known to play a key role in the partitioning of the chromosomal DNA during bacterial cell division. It appears that the C-8-methoxy moiety contributes to enhanced activity and lower selection of resistant mutants of gram-positive bacteria compared to the non-methoxy C-8 moiety. The mechanism of action of fluoroquinolones including gatifloxacin is different from that of penicillins, cephalosporins, aminoglycosides, macrolides, and tetracyclines. Therefore, fluoroquinolones may be active against pathogens that are resistant to these antibiotics. There is no cross-resistance between gatifloxacin and the mentioned classes of antibiotics. From in vitro synergy tests, gatifloxacin, as with other fluoroquinolones, is antagonistic with rifampin against enterococci. Resistance to gatifloxacin in vitro develops slowly via multiple-step mutations. Resistance to gatifloxacin in vitro occurs at a general frequency of between 1 × 10 -7 to 10 -10 . Although cross-resistance has been observed between gatifloxacin and some other fluoroquinolones, some microorganisms resistant to other fluoroquinolones may be susceptible to gatifloxacin. Gatifloxacin has been shown to be active against most strains of the following microorganisms, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section:
*Multidrug-resistant Streptococcus pneumoniae (MDRSP) includes isolates previously known as PRSP (penicillin-resistant Streptococcus pneumoniae ) and are strains resistant to two or more of the following antibiotics: penicillin (MIC >/=2 mcg/mL), 2 nd generation cephalosporins (eg, cefuroxime), macrolides, tetracyclines, and trimethoprim/sulfamethoxazole. Aerobic gram-negative microorganisms
The following in vitro data are available, but their clinical significance is unknown. Gatifloxacin exhibits in vitro minimum inhibitory concentrations (MICs) of </=2 mcg/mL against most (>/=90%) strains of the following microorganisms; however, the safety and effectiveness of gatifloxacin in treating clinical infections due to these microorganisms have not been established in adequate and well-controlled clinical trials. Aerobic gram-positive microorganisms
Aerobic gram-negative microorganisms
Anaerobic microorganisms
NOTE: The activity of gatifloxacin against Treponema pallidum has not been evaluated; however, other quinolones are not active against Treponema pallidum (see WARNINGS ). NOTE: Extended-spectrum (beta)-lactamase producing gram-negative microorganisms may have reduced susceptibility to quinolones. Susceptibility Tests Dilution techniques: Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized procedure. Standardized procedures are based on a dilution method 1 (broth or agar) or equivalent with standardized inoculum concentrations and standardized concentrations of gatifloxacin powder. The MIC values should be interpreted according to the following criteria: For testing Enterobacteriaceae and Staphylococcus species:
For testing Haemophilus influenzae and Haemophilus parainfluenzae a :
The current absence of data on resistant strains precludes defining any results other than "Susceptible". Strains yielding MIC results suggestive of a "nonsusceptible" category should be submitted to a reference laboratory for further testing. For testing Streptococcus pneumoniae b :
For testing Streptococcus species other than Streptococcus pneumoniae b :
For testing Neisseria gonorrhoeae c :
A report of "Susceptible" indicates that the pathogen is likely to be inhibited if the antimicrobial compound in the blood reaches the concentration usually achievable. A report of "Intermediate" indicates that the result should be considered equivocal, and if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where high dosage of drug can be used. This category also provides a buffer zone, which prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of "Resistant" indicates that the pathogen is not likely to be inhibited if the antimicrobial compound in the blood reaches the concentration usually achievable; other therapy should be selected. Standardized susceptibility test procedures require the use of laboratory control microorganisms to control the technical aspects of the laboratory procedures. Standard gatifloxacin powder should provide the following MIC values:
Diffusion techniques: Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure 2 requires the use of standardized inoculum concentrations. This procedure uses paper disks impregnated with 5 mcg gatifloxacin to test the susceptibility of microorganisms to gatifloxacin. Reports from the laboratory providing results of the standard single-disk susceptibility test with a 5 mcg gatifloxacin disk should be interpreted according to the following criteria: The following zone diameter interpretive criteria should be used for testing Enterobacteriaceae and Staphylococcus species:
For testing Haemophilus influenzae and Haemophilus parainflenzae g :
The current absence of data on resistant strains precludes defining any results other than "Susceptible". Strains yielding MIC results suggestive of a "nonsusceptible" category should be submitted to a reference laboratory for further testing. For testing Streptococcus pneumoniae h :
For testing Streptococcus species other than Streptococcus pneumoniae h :
For testing Neisseria gonorrhoeae i :
Interpretation should be as stated above for results using dilution techniques. Interpretation involves correlation of the diameter obtained in the disk test with the MIC for gatifloxacin. 2 As with standardized dilution techniques, methods require the use of laboratory control microorganisms that are used to control the technical aspects of the laboratory procedures. For the diffusion technique, the 5 mcg gatifloxacin disk should provide the following zone diameters in these laboratory quality control strains:
INDICATIONS AND USAGETEQUIN (gatifloxacin) is indicated for the treatment of infections due to susceptible strains of the designated microorganisms in the conditions listed below (see DOSAGE AND ADMINISTRATION ). Acute bacterial exacerbation of chronic bronchitis due to Streptococcus pneumoniae , Haemophilus influenzae , Haemophilus parainfluenzae , Moraxella catarrhalis , or Staphylococcus aureus . Acute sinusitis due to Streptococcus pneumoniae or Haemophilus influenzae . Community-acquired pneumonia due to Streptococcus pneumoniae (including multidrug-resistant strains [MDRSP]) * , Haemophilus influenzae , Haemophilus parainfluenzae , Moraxella catarrhalis , Staphylococcus aureus , Mycoplasma pneumoniae , Chlamydia pneumoniae , or Legionella pneumophila . (See Clinical Studies .) Uncomplicated skin and skin structure infections (i.e., simple abscesses, furuncles, folliculitis, wound infections, and cellulitis) due to Staphylococcus aureus (methicillin-susceptible strains only) or Streptococcus pyogenes . NOTE: An insufficient number of patients with the diagnosis of impetiginous lesions were available for evaluation. Uncomplicated urinary tract infections (cystitis) due to Escherichia coli , Klebsiella pneumoniae , or Proteus mirabilis . Complicated urinary tract infections due to Escherichia coli , Klebsiella pneumoniae , or Proteus mirabilis . Pyelonephritis due to Escherichia coli . Uncomplicated urethral and cervical gonorrhea due to Neisseria gonorrhoeae . Acute, uncomplicated rectal infections in women due to Neisseria gonorrhoeae (see WARNINGS ). To reduce the development of drug-resistant bacteria and maintain the effectiveness of TEQUIN and other antibacterial drugs, TEQUIN should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy. *Multidrug-resistant Streptococcus pneumoniae (MDRSP) includes isolates previously known as PRSP (penicillin-resistant Streptococcus pneumoniae ), and are strains resistant to two or more of the following antibiotics: penicillin (MIC >/=2 mcg/mL), 2 nd generation cephalosporins (eg, cefuroxime), macrolides, tetracyclines, and trimethoprim/sulfamethoxazole.
CONTRAINDICATIONSTEQUIN is contraindicated in persons with a history of hypersensitivity to gatifloxacin or any member of the quinolone class of antimicrobial agents.
WARNINGSTHE SAFETY AND EFFECTIVENESS OF GATIFLOXACIN IN PEDIATRIC PATIENTS, ADOLESCENTS (LESS THAN 18 YEARS OF AGE), PREGNANT WOMEN, AND LACTAT-ING WOMEN HAVE NOT BEEN ESTABLISHED (see PRECAUTIONS : Pediatric Use , Pregnancy , and Nursing Mothers ). Gatifloxacin, as with other members of the quinolone class, has caused arthropathy and/or chondrodysplasia in immature dogs. Histopathological examination of the weight-bearing joints of immature dogs revealed permanent lesions of the cartilage. The relevance of these findings to the clinical use of gatifloxacin is unknown. (See ANIMAL PHARMACOLOGY .) QTc Interval ProlongationGatifloxacin has the potential to prolong the QTc interval of the electrocardiogram in some patients. QTc prolongation may lead to an increased risk for ventricular arrhythmias including torsades de pointes. Rare cases of torsades de pointes have been spontaneously reported during postmarketing surveillance in patients receiving quinolones, including gatifloxacin. Nearly all of these rare cases were associated with one or more of the following factors: age over 60, female gender, underlying cardiac disease, and/or use of multiple medications. No cardiovascular morbidity or mortality attributable to QTc prolongation has occurred in over 44,000 patients treated with gatifloxacin in clinical trials; these include 118 patients concurrently receiving drugs known to prolong the QTc interval and 139 patients known to have uncorrected hypokalemia (ECG monitoring was not performed). Gatifloxacin should be avoided in patients with known prolongation of the QTc interval, patients with uncorrected hypokalemia, and patients receiving class IA (quinidine, procainamide), or class III (amiodarone, sotalol) antiarrhythmic agents. (See CLINICAL PHARMACOLOGY : Electrocardiogram .) Pharmacokinetic and pharmacodynamic studies between gatifloxacin and drugs that prolong the QTc interval such as cisapride, erythromycin, antipsychotics, and tricyclic antidepressants have not been performed. Gatifloxacin should be used with caution when given concurrently with these drugs, as well as in patients with ongoing proarrhythmic conditions, such as clinically significant bradycardia or acute myocardial ischemia. The magnitude of QTc prolongation increases with increasing concentrations of the drug (see CLINICAL PHARMACOLOGY : Electrocardiogram ); therefore, the recommended dose and the recommended intravenous infusion rate should not be exceeded (see DOSAGE AND ADMINISTRATION for dosing recommendations for patients with or without renal impairment). Disturbances in Blood GlucoseDisturbances of blood glucose, including symptomatic hyper- and hypoglycemia, have been reported with TEQUIN, usually in diabetic patients. Therefore, careful monitoring of blood glucose is recommended when TEQUIN is administered to patients with diabetes (see CLINICAL PHARMACOLOGY , PRECAUTIONS : Information for Patients and Drug Interactions , and ANIMAL PHARMACOLOGY ). Studies conducted in non-infected patients with type 2 diabetes mellitus controlled on oral hypoglycemic agents have demonstrated that TEQUIN is associated with disturbances in glucose homeostasis including an increase in serum insulin and decrease in serum glucose usually following administration of initial doses (i.e., first 2 days of treatment), and sometimes associated with symptomatic hypoglycemia. Increases in fasting serum glucose were also observed, usually after the third day of TEQUIN (gatifloxacin) administration, continuing throughout the duration of treatment, and returning to baseline by 28 days after the cessation of gatifloxacin treatment in most patients. During the postmarketing period, there have been reports of serious disturbances of glucose homeostasis in patients being treated with TEQUIN. Hypoglycemic episodes, in some cases severe, have been reported in patients with diabetes mellitus treated with either sulfonylurea or non-sulfonylurea oral hypoglycemic medications. These events frequently occurred on the first day of therapy and usually within 3 days following the initiation of TEQUIN. Hyperglycemic episodes, in some cases severe and associated with hyperosmolar non-ketotic hyperglycemic coma, were reported in diabetic patients, mostly between 4 and 10 days following the initiation of TEQUIN therapy. Some of the hyperglycemic and hypoglycemic events were life-threatening and many required hospitalization, although these events were reversible when appropriately managed. Many of these patients had other underlying medical problems and were receiving concomitant medications that may have contributed to the glucose abnormality. Episodes of hyperglycemia, including hyperosmolar non-ketotic hyperglycemic coma, also occurred in patients not previously diagnosed with diabetes mellitus. Elderly patients who may have unrecognized diabetes, age-related decrease in renal function, underlying medical problems, and/or are taking concomitant medications associated with hyperglycemia may be at particular risk for serious hyperglycemia. The dose of TEQUIN should be adjusted based on underlying renal function (see DOSAGE AND ADMINISTRATION ). When TEQUIN is used in diabetic patients, blood glucose should be closely monitored. Signs and symptoms of hypoglycemia should be monitored, especially during the first 3 days of therapy, and signs and symptoms of hyperglycemia should be monitored in diabetics and patients who may be at risk for hyperglycemia, especially with continued treatment with TEQUIN beyond 3 days. If signs and symptoms of either hypoglycemia or hyperglycemia occur in any patient being treated with TEQUIN, appropriate therapy must be initiated immediately and TEQUIN should be discontinued. Tendon EffectsRuptures of the shoulder, hand, and Achilles tendon or other tendons that required surgical repair or resulted in prolonged disability have been reported in patients receiving quinolones, including gatifloxacin. Postmarketing surveillance reports indicate that this risk may be increased in patients receiving concomitant corticosteroids, especially the elderly. Gatifloxacin should be discontinued if the patient experiences pain, inflammation, or rupture of a tendon. Patients should rest and refrain from exercise until the diagnosis of tendonitis or tendon rupture has been excluded. Tendon rupture can occur during or after therapy with quinolones, including gatifloxacin. Peripheral NeuropathyRare cases of sensory or sensorimotor axonal polyneuropathy affecting small and/or large axons resulting in paresthesias, hypoesthesias, dysesthesias and weakness have been reported in patients receiving quinolones. OtherConvulsions, increased intracranial pressure, and psychosis have been reported in patients receiving quinolones. Quinolones may also cause central nervous system (CNS) stimulation, which may lead to tremors, restlessness, lightheadedness, confusion, hallucinations, paranoia, depression, nightmares, and insomnia. These reactions may occur following the first dose. If these reactions occur in patients receiving gatifloxacin, the drug should be discontinued and appropriate measures instituted (see ADVERSE REACTIONS ). As with other quinolones, TEQUIN should be used with caution in patients with known or suspected CNS disorders, such as severe cerebral atherosclerosis, epilepsy, and other factors that predispose to seizures. Serious and occasionally fatal hypersensitivity and/or anaphylactic reactions have been reported in patients receiving therapy with quinolones. These reactions may occur following the first dose. Some reactions have been accompanied by cardiovascular collapse, hypotension/shock, seizure, loss of consciousness, tingling, angioedema (including tongue, laryngeal, throat or facial edema/swelling), airway obstruction (including bronchospasm, shortness of breath, and acute respiratory distress), dyspnea, urticaria, itching and other serious skin reactions. TEQUIN should be discontinued at the first appearance of a skin rash or any other sign of hypersensitivity. Serious acute hypersensitivity reactions may require treatment with epinephrine and other resuscitative measures, including oxygen, intravenous fluids, antihistamines, corticosteroids, pressor amines, and airway management, as clinically indicated (see PRECAUTIONS ). Serious and sometimes fatal events, some due to hypersensitivity and some due to uncertain etiology, have been reported in patients receiving antibacterial therapy. These events may be severe and generally occur following the administration of multiple doses. Clinical manifestations may include one or more of the following: fever, rash or severe dermatologic reactions (eg, toxic epidermal necrolysis, Stevens-Johnson syndrome); vasculitis, arthralgia, myalgia, serum sickness; allergic pneumonitis, interstitial nephritis; acute renal insufficiency or failure; hepatitis, jaundice, acute hepatic necrosis or failure; anemia, including hemolytic and aplastic; thrombocytopenia, including thrombotic thrombocytopenic purpura; leukopenia; agranulocytosis; pancytopenia; and/or other hematologic abnormalities. Pseudomembranous colitis has been reported with nearly all antibacterial agents, including TEQUIN, and may range in severity from mild to life-threatening. It is important, therefore, to consider this diagnosis in patients who present with diarrhea subsequent to the administration of any antibacterial agent. Treatment with antibacterial agents alters the flora of the colon and may permit overgrowth of clostridia. Studies indicate that a toxin produced by Clostridium difficile is the primary cause of "antibiotic-associated colitis." After the diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to drug discontinuation alone. In moderate to severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation, and treatment with an antibacterial drug clinically effective against C. difficile colitis. Gatifloxacin has not been shown to be effective in the treatment of syphilis. Antimicrobial agents used in high doses for short periods of time to treat gonorrhea may mask or delay the symptoms of incubating syphilis. All patients with gonorrhea should have a serologic test for syphilis at the time of diagnosis.
PRECAUTIONSGeneralPrescribing TEQUIN in the absence of proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria. Quinolones may cause central nervous system (CNS) events including nervousness, agitation, insomnia, anxiety, nightmares, or paranoia (see WARNINGS and PRECAUTIONS: Information for Patients ). Administer gatifloxacin with caution in the presence of renal insufficiency. Careful clinical observation and appropriate laboratory studies should be performed prior to and during therapy since elimination of gatifloxacin may be reduced. In patients with impaired renal function (creatinine clearance <40 mL/min), adjustment of the dosage regimen is necessary to avoid the accumulation of gatifloxacin due to decreased clearance (see CLINICAL PHARMACOLOGY and DOSAGE AND ADMINISTRATION ). Because a hypotonic solution results, Water for Injection should not be used as a diluent when preparing a 2 mg/mL solution from the concentrated solution of gatifloxacin (10 mg/mL) (see DOSAGE AND ADMINISTRATION ). Disturbances of blood glucose homeostasis have been reported during the postmarketing period (see CLINICAL PHARMACOLOGY , WARNINGS , and ANIMAL PHARMACOLOGY ). Information for Patients (See Patient Information Section.) To assure safe and effective use of TEQUIN, the following information and instructions should be communicated to the patient when appropriate. Patients should be advised:
Drug InteractionsTEQUIN (gatifloxacin) can be taken 4 hours before ferrous sulfate, dietary supplements containing zinc, magnesium, or iron (such as multivitamins), or aluminum/magnesium-containing antacids without any significant pharmacokinetic interactions (see CLINICAL PHARMACOLOGY ). Milk, calcium carbonate, cimetidine, theophylline, warfarin, or midazolam: No significant interactions have been observed when administered concomitantly with TEQUIN. No dosage adjustments are necessary when these drugs are administered concomitantly with TEQUIN (see CLINICAL PHARMACOLOGY ). Antidiabetic Agents: Pharmacodynamic changes in glucose homeostasis have been seen with concomitant glyburide use. However, no significant pharmacokinetic interactions have been observed when glyburide was administered concomitantly with TEQUIN (see CLINICAL PHARMACOLOGY: Glucose Homeostasis and WARNINGS ). Digoxin: Concomitant administration of TEQUIN and digoxin did not produce significant alteration of the pharmacokinetics of gatifloxacin; however, an increase in digoxin concentrations was observed for 3 of 11 subjects. Patients taking digoxin should therefore be monitored for signs and/or symptoms of toxicity. In patients who display signs and/or symptoms of digoxin intoxication, serum digoxin concentrations should be determined, and digoxin dosage should be adjusted as appropriate (see CLINICAL PHARMACOLOGY ). Probenecid: The systemic exposure of TEQUIN is significantly increased following the concomitant administration of TEQUIN and probenecid (see CLINICAL PHARMACOLOGY ). Warfarin: In subjects receiving warfarin, no significant change in clotting time was observed when gatifloxacin was coadministered. However, because some quinolones have been reported to enhance the effects of warfarin or its derivatives, prothrombin time or other suitable anticoagulation test should be monitored closely if a quinolone antimicrobial is administered with warfarin or its derivatives. Nonsteroidal anti-inflammatory drugs (NSAIDS): Although not observed with gatifloxacin in preclinical and clinical trials, the concomitant administration of nonsteroidal anti-inflammatory drugs with a quinolone may increase the risks of CNS stimulation and convulsions (see WARNINGS ). Laboratory Test InteractionsThere are no reported laboratory test interactions. Carcinogenesis, Mutagenesis, Impairment of FertilityB6C3F1 mice given gatifloxacin in the diet for 18 months at doses with an average intake of up to 81 mg/kg/day in males and 90 mg/kg/day in females showed no increases in neoplasms. These doses are approximately 0.13 and 0.18 times the maximum recommended human dose based upon daily systemic exposure (AUC). In a 2-year dietary carcinogenicity study in Fischer 344 rats, no increases in neoplasms were seen in males given doses up to 47 mg/kg/day and females given up to 139 mg/kg/day. These doses are approximately 0.36 (males) and 0.81 (females) times the maximum recommended human dose based upon daily systemic exposure. A statistically significant increase in the incidence of large granular lymphocyte (LGL) leukemia was seen in males treated with a high dose of 100 mg/kg/day (approximately 0.74 times the maximum recommended human dose based upon daily systemic exposure) versus controls. Although Fischer 344 rats have a high spontaneous background rate of LGL leukemia, the incidence in high-dose males slightly exceeded the historical control range established for this strain. The findings in high-dose males are not considered a concern with regard to the safe use of gatifloxacin in humans. In genetic toxicity tests, gatifloxacin was not mutagenic in several strains of bacteria used in the Ames test; however, it was mutagenic to Salmonella strain TA102. Gatifloxacin was negative in four in vivo assays that included oral and intravenous micronucleus tests in mice, an oral cytogenetics test in rats, and an oral DNA repair test in rats. Gatifloxacin was positive in in vitro gene-mutation assays in Chinese hamster V-79 cells and in vitro cytogenetics assays in Chinese hamster CHL/IU cells. These findings were not unexpected; similar findings have been seen with other quinolones and may be due to the inhibitory effects of high concentrations on eukaryotic type II DNA topoisomerase. There were no adverse effects on fertility or reproduction in rats given gatifloxacin orally at doses up to 200 mg/kg/day (approximately equivalent to the maximum human dose based on systemic exposure [AUC]). Pregnancy: Category CThere were no teratogenic effects observed in rats or rabbits at oral gatifloxacin doses up to 150 or 50 mg/kg, respectively (approximately 0.7 and 1.9 times the maximum human dose based on systemic exposure). However, skeletal malformations were observed in fetuses from rats given 200 mg/kg/day orally or 60 mg/kg/day intravenously during organogenesis. Developmental delays in skeletal ossification, including wavy ribs, were observed in fetuses from rats given oral doses of >/=150 mg/kg or intravenous doses of >/=30 mg/kg daily during organogenesis, suggesting that gatifloxacin is slightly fetotoxic at these doses. Similar findings have been seen with other quinolones. These changes were not seen in rats or rabbits given oral doses of gatifloxacin up to 50 mg/kg (approximately 0.2 and 1.9 times the maximum human dose, respectively, based on systemic exposure). When rats were given oral doses of 200 mg/kg of gatifloxacin beginning in late pregnancy and continuing throughout lactation, late postimplantation loss increased, as did neonatal and perinatal mortalities. These observations also suggest fetotoxicity. Similar findings have been seen with other quinolones. Because there are no adequate and well-controlled studies in pregnant women, TEQUIN should be used during pregnancy only if the potential benefit outweighs the potential risk to the fetus. Nursing MothersGatifloxacin is excreted in the breast milk of rats. It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when gatifloxacin is administered to a nursing woman. Pediatric UseThe safety and effectiveness of gatifloxacin in pediatric patients less than 18 years of age have not been established. Gatifloxacin, similar to other quinolones, causes arthropathy and permanent histological changes in weight-bearing joints of juvenile animals (see WARNINGS and ANIMAL PHARMACOLOGY ). Geriatric UseDuring the postmarketing period, serious disturbances of glucose homeostasis have been reported in elderly patients being treated with TEQUIN (see WARNINGS , PRECAUTIONS: Drug Interactions and ANIMAL PHARMACOLOGY ). In multiple-dose clinical trials of gatifloxacin (n=2891), 22% of patients were >/=65 years of age and 10% were >/=75 years of age. No overall differences in safety or efficacy were observed in clinical trials between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function (see DOSAGE AND ADMINISTRATION ).
ADVERSE REACTIONSOver 5000 patients have been treated with gatifloxacin in single- and multiple-dose clinical efficacy trials worldwide. In gatifloxacin studies, the majority of adverse reactions were described as mild in nature. Gatifloxacin was discontinued for adverse events thought related to drug in 2.7% of patients. Drug-related adverse events classified as possibly, probably, or definitely related with a frequency of >/=3% in patients receiving gatifloxacin in single- and multiple-dose clinical trials are as follows: nausea 8%, vaginitis 6%, diarrhea 4%, headache 3%, dizziness 3%. In patients who were treated with either intravenous gatifloxacin or with intravenous followed by oral therapy, the incidence of adverse events was similar to those who received oral therapy alone. Local injection site reactions (redness at injection site) were noted in 5% of patients. Additional drug-related adverse events (possibly, probably, or definitely related) considered clinically relevant that occurred in >/=0.1% to <3% of patients receiving gatifloxacin in single- and multiple-dose clinical trials are as follows:
Laboratory ChangesClinically relevant changes in laboratory parameters, without regard to drug relationship, occurred in fewer than 1% of TEQUIN (gatifloxacin)-treated patients. These included the following: neutropenia, increased ALT or AST levels, alkaline phosphatase, bilirubin, serum amylase, and electrolytes abnormalities. It is not known whether these abnormalities were caused by the drug or the underlying condition being treated. Postmarketing Adverse Event ReportsThe following events have been reported during post-approval use of TEQUIN. Because these events are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Abnormal renal function (including acute renal failure), acute allergic reaction including anaphylactic reaction and angioneurotic edema, hepatitis, hypotension, increased International Normalized Ratio (INR)/prothrombin time, pancreatitis, severe hyperglycemia (including hyperosmolar nonketotic hyperglycemia), severe hypoglycemia (including hypoglycemic coma), Stevens-Johnson syndrome, syncope, tendon rupture, thrombocytopenia, and torsades de pointes.
OVERDOSAGEGatifloxacin exhibits a low potential for acute toxicity in animal studies. The minimum lethal oral doses in rats and dogs were greater than 2000 mg/kg and 1000 mg/kg, respectively. The minimum lethal intravenous dose was 144 mg/kg in rats and greater than 45 mg/kg in dogs. Clinical signs observed included decreased activity and respiratory rate, vomiting, tremors, and convulsions. In the event of acute oral overdose, the stomach should be emptied by inducing vomiting or by gastric lavage. The patient should be carefully observed (including ECG monitoring) and given symptomatic and supportive treatment. Adequate hydration should be maintained. Gatifloxacin is not efficiently removed from the body by hemodialysis (approximately 14% recovered over 4 hours) or by chronic ambulatory peritoneal dialysis (CAPD) (approximately 11% recovered over 8 days).
DOSAGE AND ADMINISTRATIONThe recommended dosage for TEQUIN Tablets or TEQUIN Injection is described in Table 4. Doses of TEQUIN are administered once every 24 hours. These recommendations apply to all patients with a creatinine clearance >/=40 mL/min. For patients with a creatinine clearance <40 mL/min, see the Impaired Renal Function subsection. TEQUIN can be administered without regard to food, including milk and dietary supplements containing calcium. Oral doses of TEQUIN should be administered at least 4 hours before the administration of ferrous sulfate, dietary supplements containing zinc, magnesium, or iron (such as multivitamins), aluminum/magnesium-containing antacids, or VIDEX ® (didanosine) buffered tablets or pediatric powder for oral solution. TEQUIN can be administered without regard to gender or age (>/=18 years). Consideration should be given to the possibility that the elderly may have impaired renal function (see PRECAUTIONS : Geriatric Use ). When switching from intravenous to oral dosage administration, no dosage adjustment is necessary. Patients whose therapy is started with TEQUIN Injection may be switched to TEQUIN Tablets when clinically indicated at the discretion of the physician. TEQUIN Injection should be administered by INTRAVENOUS infusion only. It is not intended for intramuscular, intrathecal, intraperitoneal, or subcutaneous administration. Single-use vials require dilution prior to administration. (See Preparation of Gatifloxacin for Intravenous Administration .) TEQUIN Injection should be administered by intravenous infusion over a period of 60 minutes. CAUTION: RAPID OR BOLUS INTRAVENOUS INFUSION SHOULD BE AVOIDED.
Impaired Renal FunctionSince gatifloxacin is eliminated primarily by renal excretion, a dosage modification of TEQUIN is recommended for patients with creatinine clearance <40 mL/min, including patients on hemodialysis and on CAPD. The recommended dosage of TEQUIN (gatifloxacin) is:
Administer TEQUIN (gatifloxacin) after a dialysis session for patients on hemodialysis. Single 400 mg dose TEQUIN regimen (for the treatment of uncomplicated urinary tract infections and gonorrhea) and 200 mg once daily for 3 days TEQUIN regimen (for the treatment of uncomplicated urinary tract infections) require no dosage adjustment in patients with impaired renal function. The following formula may be used to estimate creatinine clearance:
Chronic Hepatic DiseaseNo adjustment in the dosage of TEQUIN is necessary in patients with moderate hepatic impairment (Child-Pugh Class B). There are no data in patients with severe hepatic impairment (Child-Pugh Class C) (see CLINICAL PHARMACOLOGY ). Intravenous AdministrationPreparation of Gatifloxacin for Intravenous AdministrationTEQUIN solution in single-use vials: TEQUIN Injection is supplied in single-use 40-mL vials (10 mg/mL) containing a concentrated solution of gatifloxacin in 5% dextrose (400 mg of gatifloxacin) (see HOW SUPPLIED ). THESE TEQUIN INJECTION SINGLE-USE VIALS MUST BE FURTHER DILUTED WITH AN APPROPRIATE SOLUTION PRIOR TO INTRAVENOUS ADMINISTRATION. The concentration of the resulting diluted solution should be 2 mg/mL prior to administration. Compatible intravenous solutions: Because a hypotonic solution results, Water for Injection should not be used as a diluent when preparing a 2 mg/mL solution from the concentrated solution of gatifloxacin (10 mg/mL) (see PRECAUTIONS ). Any of the following intravenous solutions may be used to prepare a 2 mg/mL gatifloxacin solution:
Plasma-Lyte ® 56 and 5% Dextrose Injection (Multiple Electrolytes and Dextrose Injection, Type 1, USP) M/6 Sodium Lactate Injection, USP
Plasma-Lyte ® is a registered trademark of Baxter International, Inc. Gatifloxacin solutions at 2 mg/mL also have been shown to be compatible with 20 mEq/L Potassium Chloride in 5% Dextrose and 0.45% Sodium Chloride Injection, USP. This intravenous drug product should be inspected visually for particulate matter prior to dilution and administration. Samples containing visible particles should be discarded. Since no preservative or bacteriostatic agent is present in this product, aseptic technique must be used in preparation of the final intravenous solution. Since the vials are for single-use only, any unused portion remaining in the vial should be discarded. Since only limited data are available on the compatibility of gatifloxacin intravenous injection with other intravenous substances, additives or other medications should not be added to TEQUIN Injection in single-use vials or infused simultaneously through the same intravenous line. If the same intravenous line is used for sequential infusion of different drugs, the line should be flushed before and after infusion of TEQUIN Injection with an infusion solution compatible with TEQUIN Injection and with any other drug(s) administered via this common line. If TEQUIN Injection is to be given concomitantly with another drug, each drug should be given separately in accordance with the recommended dosage and route of administration for each drug. TEQUIN Injection premix in single-use flexible containers: TEQUIN Injection is also available in ready-to-use 100- and 200-mL flexible bags containing a dilute solution of 200 or 400 mg gatifloxacin in 5% dextrose. NO FURTHER DILUTION OF THIS PREPARATION IS NECESSARY. This intravenous drug product should be inspected visually for particulate matter prior to administration. Samples containing visible particles should be discarded. Since the premix flexible bags are for single use only, any unused portion should be discarded. Since only limited data are available on the compatibility of gatifloxacin intravenous injection with other intravenous substances, additives or other medications should not be added to TEQUIN Injection in flexible containers or infused simultaneously through the same intravenous line. If the same intravenous line is used for sequential infusion of different drugs, the line should be flushed before and after infusion of TEQUIN Injection with an infusion solution compatible with TEQUIN Injection and with any other drug(s) administered via this common line. Instructions for the use of TEQUIN (gatifloxacin in 5% dextrose) Injection premix in flexible containers: To open:
Preparation for administration:
Stability of TEQUIN Injection as Supplied When stored under recommended conditions, TEQUIN Injection, as supplied in 40-mL vials and in 100-mL and 200-mL flexible containers, is stable through the expiration date printed on the label. Stability of TEQUIN Injection Following Dilution TEQUIN Injection, when diluted in a compatible intravenous fluid to a concentration of 2 mg/mL, is stable for 14 days when stored between 20°C to 25°C or when stored under refrigeration between 2°C to 8°C. TEQUIN Injection, when diluted to a concentration of 2 mg/mL in a compatible intravenous fluid EXCEPT FOR 5% SODIUM BICARBONATE INJECTION, USP, may be stored for up to 6 months at -25°C to -10°C (-13°F to 14°F). Frozen solutions may be thawed at controlled room temperature. Solutions that have been thawed are stable for 14 days after removal from the freezer when stored between 20°C to 25°C or when stored under refrigeration between 2°C to 8°C. Solutions should not be refrozen.
HOW SUPPLIEDTablets TEQUIN ® (gatifloxacin) Tablets are available as 200-mg and 400-mg white, film-coated tablets. The tablets are almond shaped and biconvex and contain gatifloxacin sesquihydrate equivalent to either 200 mg or 400 mg gatifloxacin. TEQUIN Tablets are packaged in bottles, unit dose blister strips, and multidose blister packs of 5 tablets (TEQUIN Teq-Paq™) in the following configurations: 200-mg tablets -- color: white; shape: biconvex; debossing: "BMS" on one side and "TEQUIN" and "200" on the other.
400-mg tablets -- color: white; shape: biconvex; debossing: "BMS" on one side and "TEQUIN" and "400" on the other.
Carton of 3 TEQUIN Teq-Paq™ (5 tablets each) (NDC 0015-1177-21) Storage Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature]. Intravenous Solution -- Single-Use Vials TEQUIN ® (gatifloxacin) Injection is available for intravenous administration in the following configuration: Single-use vials containing a clear, light yellow to greenish-yellow solution at a concentration of 10 mg/mL gatifloxacin.
Storage Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature]. Intravenous Solution -- Premix Bags TEQUIN ® (gatifloxacin in 5% dextrose) Injection is available in ready-to-use flexible bags containing a dilute solution of 200 mg or 400 mg of gatifloxacin in 5% dextrose. Premix bags are manufactured by Baxter Healthcare Corp., Deerfield, IL 60015 USA. 2-mg/mL (200-mg), 100-mL flexible container, carton of 24 (NDC 0015-1180-78) 2-mg/mL (400-mg), 200-mL flexible container, carton of 24 (NDC 0015-1181-78) Storage Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature]. Do not freeze.
ANIMAL PHARMACOLOGYIn three animal species (rats, beagle dogs, and cynomolgus monkeys) given oral gatifloxacin doses approximately 1.0- to 19-times the approved human dose (based on body surface area) from one to six months, electron microscopy showed vesiculation of rough endoplasmic reticulum and decreased secretory granules in pancreatic (beta)-cells of all three species. These ultrastructural changes correlated with vacuolation of pancreatic (beta)-cells seen by light microscopy in dogs given a dose level for one or six months that was approximately equivalent to the human dose (based upon body surface area and plasma AUC). Following a 4-week recovery period without gatifloxacin, partial recovery from these pancreatic changes was seen in the rat, and complete recovery was evident in beagle dogs and cynomolgus monkeys (see WARNINGS and CLINICAL PHARMACOLOGY ). In contrast to some other quinolone antibacterials, there was no evidence of phototoxicity when gatifloxacin was evaluated in the hairless mouse or guinea pig models using simulated sunlight or UVA radiation, respectively. Unlike some other members of the quinolone class, crystalluria, ocular toxicity, and testicular degeneration were not observed in 6-month repeat dose studies with rats or dogs given gatifloxacin. While some quinolone antibacterials have proconvulsant activity that is exacerbated with concomitant use of nonsteroidal anti-inflammatory drugs (NSAID), gatifloxacin did not produce an increase in seizure activity when administered intravenously to mice at doses up to 100 mg/kg in combination with the NSAID fenbufen. Quinolone antibacterials have been shown to cause arthropathy in immature animals. There is no evidence of arthropathy in fully mature rats and dogs given gatifloxacin for 6 months at doses of 240 or 24 mg/kg, respectively (approximately 1.5 times the maximum human dose in both species based on systemic exposure). Arthropathy and chondrodysplasia were observed in immature dogs given 10 mg/kg gatifloxacin orally for 7 days (approximately equal to the maximum human dose based upon systemic exposure) [see WARNINGS ]. The relevance of these findings to the clinical use of gatifloxacin is unknown. In an additional study in immature dogs given gatifloxacin orally for 2 weeks with a 6-month recovery period, articular cartilage lesions were observed at >/=5 mg/kg (approximately 0.3 times human therapeutic dose levels based on plasma AUC comparisons), and growth plate cartilage lesions were seen at 10 and 20 mg/kg (approximately equivalent to human therapeutic dose levels based on plasma AUC comparisons). Articular cartilage changes seen on gross pathology and histopathology persisted through the 6-month recovery period, whereas growth plate cartilage lesions were resolved. (See WARNINGS .) The relevance of these findings to the clinical use of gatifloxacin is unknown. Some members of the quinolone class have been shown to cause prolongation of the QT interval in dogs. Intravenous 10-mg/kg bolus doses of gatifloxacin had no effect on QT interval in anesthetized dogs.
CLINICAL STUDIESCommunity-Acquired Bacterial Pneumonia and Community-Acquired Pneumonia Due to Multidrug-Resistant Streptococcus pneumoniae (MDRSP) *Clinical efficacy of gatifloxacin in the treatment of community-acquired bacterial pneumonia (CAP) was evaluated in two non-comparative Phase II/III studies and three Phase III studies comparing oral TEQUIN to oral clarithromycin, TEQUIN IV/oral to levofloxacin IV/oral, and TEQUIN IV/oral to ceftriaxone IV (+/- erythromycin IV) with step-down to oral clarithromycin. Success rates for clinically evaluable patients with a bacterial pathogen isolated at baseline (see INDICATIONS AND USAGE ) ranged from 88% to 90% for TEQUIN-treated patients. Success rates were not statistically different from comparator therapy. Gatifloxacin was also effective for the treatment of community-acquired pneumonia caused by multidrug-resistant Streptococcus pneumoniae (MDRSP * ) isolates. Of 27 clinically and microbiologically evaluable patients with MDRSP isolates obtained primarily from post-marketing studies of patients with CAP, 100% achieved clinical and bacteriological success post-therapy. The clinical cure rates and bacteriological success rates are shown in the table below. *Multidrug-resistant Streptococcus pneumoniae (MDRSP) includes isolates previously known as PRSP (penicillin-resistant Streptococcus pneumoniae ) and are strains resistant to two or more of the following antibiotics: penicillin (MIC >/=2 mcg/mL), 2 nd generation cephalosporins (eg, cefuroxime), macrolides, tetracyclines, and trimethoprim/sulfamethoxazole.
Not all isolates were resistant to all antimicrobial classes tested. Success and eradication rates are summarized in the table below.
REFERENCES
Patient Information About:TEQUIN ® (gatifloxacin) 200-mg and 400-mg Tablets This section contains important information about TEQUIN (gatifloxacin) that you should read before you begin treatment. This section does not list all the benefits and risks of TEQUIN and does not take the place of discussions with your doctor or healthcare professional about your medical condition or your treatment. If you have questions, talk with your healthcare professional. The medicine described here can only be prescribed by a licensed healthcare professional. Only your healthcare professional can determine if TEQUIN is right for you. What is TEQUIN? TEQUIN ( pronounced TEK win ) is an antibiotic used to treat lung, sinus, skin, or urinary tract infections, and also to treat certain sexually transmitted diseases caused by germs called bacteria. TEQUIN kills many of the kinds of bacteria that can infect the lungs, sinus, skin, and urinary tract and that cause certain sexually transmitted diseases. TEQUIN has been shown in a large number of clinical trials to be safe and effective for the treatment of bacterial infections. Sometimes viruses, rather than bacteria, may infect the lungs and sinuses (for example, the common cold). TEQUIN, like all other antibiotics, does not kill viruses. The sexually transmitted disease called gonorrhea is treated by TEQUIN. Other diseases called syphilis or non-gonococcal disease are not treated by TEQUIN. You should contact your doctor if you think your condition is not improving while taking TEQUIN. TEQUIN tablets are white and contain either 200 mg or 400 mg of active drug. How and when should I take TEQUIN?TEQUIN should be taken once a day for 1 to 14 days depending on your prescription. It should be swallowed whole and may be taken with or without food. Try to take the tablet at the same time each day. You may begin to feel better quickly; however, in order to make sure that all bacteria are killed, you should complete the full course of medication. Do not take more than the prescribed dose of TEQUIN. Try not to miss a dose, but if you do, take it as soon as possible. If it is almost time for the next dose, skip the missed dose and continue your regular dose. Who should not take TEQUIN?You should avoid TEQUIN if you have ever had a severe allergic reaction to any medicine in the group of antibiotics known as "quinolones" such as AVELOX ® (moxifloxacin hydrochloride), CIPRO ® (ciprofloxacin) or LEVAQUIN ® (levofloxacin). You should avoid TEQUIN if you have a rare condition known as congenital prolongation of the QTc interval. If any of your family members have this condition, you should inform your healthcare professional. You should avoid TEQUIN if you are being treated for heart rhythm disturbances with certain medicines such as quinidine, procainamide, amiodarone, or sotalol. Inform your healthcare professional if you are taking a heart rhythm drug. You should avoid TEQUIN if you have a condition known as hypokalemia (low blood potassium). Hypokalemia may be caused by medicines called diuretics such as furosemide and hydrochlorothiazide. If you are taking a diuretic you should speak with your healthcare professional. If you are pregnant or planning to become pregnant while taking TEQUIN, talk to your doctor before taking this medication. TEQUIN is not recommended for use during pregnancy or nursing, as the effects on the unborn child or nursing infant are unknown. TEQUIN is not recommended for children. What about other medications I am taking?It is important to let your healthcare provider know all of the medicines that you are using.
What are the possible side effects of TEQUIN?TEQUIN is generally well tolerated. The most common side effects that can occur when taking TEQUIN are usually mild and include nausea, vomiting, stomach ache, diarrhea, dizziness, and headache. You should be careful about driving or operating machinery until you are sure TEQUIN does not cause dizziness. If you notice any side effects not mentioned in this section or if you have any questions or concerns about the side effects you are experiencing, please discuss them with your healthcare professional. In a few people, TEQUIN, like some other antibiotics, may produce a small effect on the heart that is seen on an electrocardiogram test. Although this did not cause any problems in patients who took TEQUIN in premarketing clinical trials, in theory, it could result in extremely rare cases of abnormal heartbeat, which may be dangerous. Contact your healthcare professional if you develop heart palpitations (fast beating) or have fainting spells. Disturbances of blood sugar, including symptoms of high blood sugar (hyperglycemia) and low blood sugar (hypoglycemia), have been reported with TEQUIN in diabetic patients. Elderly patients with additional medical problems or taking additional medications may also be at risk for high blood sugar. If you develop low blood sugar while on TEQUIN, you should take immediate measures to increase your blood sugar, stop taking TEQUIN, and contact your healthcare professional at once. If you develop high blood sugar while on TEQUIN, you should contact your healthcare professional at once before taking additional TEQUIN. If you have diabetes or suspect that you may have diabetes, discuss how to detect changes in your blood sugar with your healthcare professional at once before taking additional TEQUIN. Where can I get more information about TEQUIN?This section is a summary of the most important information about TEQUIN. It does not include everything there is to know about TEQUIN. If you have any questions or problems, you should talk to your doctor or healthcare provider. There is also a leaflet (Package Insert) written for healthcare professionals that your pharmacist can let you read. You may want to read this information and discuss it with your doctor or other healthcare professional. Remember, no written information can replace careful discussion with your doctor. Remember
VIDEX ® (didanosine) is a registered trademark of Bristol-Myers Squibb Company. Other brands are the trade-marks of their respective owners and are not trademarks of Bristol-Myers Squibb Company. Bristol-Myers Squibb Company Princeton, NJ 08543 U.S.A. E5-B0001-05-05 Revised May 2005 Based on 51-029012-03, 1188383A1 Licensed from Kyorin Pharmaceutical Company, Limited, Tokyo, Japan
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 - To bookmark this page (add it to your favorites), please click the image to the left.
- To bookmark this page (add it to your favorites), please click the image to the left.