| DRUGS INDEX | MANUFACTURERS INDEX | ANATOMY | GEOGRAPHY | USA STATISTICS | CHINA STATISTICS | RELIGION | JOBS |
 |
||
Tylenol with Codeine Elixir, Tylenol with Codeine Tablets (Ortho-Mcneil) | ||
|
- Drugs index - Manufacturers - Feedback 
|
Prescribing InformationDESCRIPTIONEach tablet contains: No. 3 Codeine Phosphate .............. 30 mg Acetaminophen ........................... 300 mg No. 4 Codeine Phosphate ............... 60 mg Acetaminophen ........................... 300 mg Inactive ingredients: powdered cellulose, magnesium stearate, sodium metabisulfite **/* , pregelatinized starch, starch (corn). Acetaminophen, 4'-hydroxyacetanilide, is a nonopiate, non-salicylate analgesic and antipyretic which occurs as a white, odorless, crystalline powder, possessing a slightly bitter taste. Its structure is as follows:
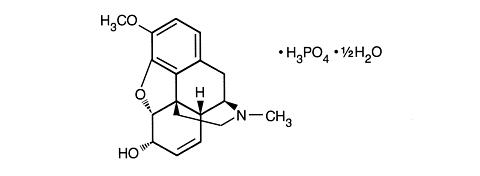
C 8 H 9 NO 2 M.W. 151.16 Codeine is an alkaloid, obtained from opium or prepared from morphine by methylation. Codeine phosphate occurs as fine, white, needle-shaped crystals, or white, crystalline powder. It is affected by light. Its chemical name is: 7,8-didehydro- 4,5(alpha)-epoxy-3-methoxy-17-methylmorphinan-6(alpha)-ol phosphate (1:1) (salt) hemihydrate. Its structure is as follows:
C 18 H 21 NO 3 .H 3 PO 4 . 1 / 2 H 2 O M.W. 406.37 **/* See WARNINGS
CLINICAL PHARMACOLOGYTYLENOL® with Codeine (acetaminophen and codeine phosphate) tablets combine the analgesic effects of a centrally acting analgesic, codeine, with a peripherally acting analgesic, acetaminophen. Both ingredients are well absorbed orally. The plasma elimination half-life ranges from 1 to 4 hours for acetaminophen, and from 2.5 to 3 hours for codeine. Codeine retains at least one-half of its analgesic activity when administered orally. A reduced first-pass metabolism of codeine by the liver accounts for the greater oral efficacy of codeine when compared to most other morphine-like narcotics. Following absorption, codeine is metabolized by the liver and metabolic products are excreted in the urine. Approximately 10 percent of the administered codeine is demethylated to morphine, which may account for its analgesic activity. Acetaminophen is distributed throughout most fluids of the body, and is metabolized primarily in the liver. Little unchanged drug is excreted in the urine, but most metabolic products appear in the urine within 24 hours.
INDICATIONS AND USAGETYLENOL® with Codeine (acetaminophen and codeine phosphate) tablets are indicated for the relief of mild to moderately severe pain.
CONTRAINDICATIONSTYLENOL® with Codeine (acetaminophen and codeine phosphate) tablets should not be administered to patients who have previously exhibited hypersensitivity to any component.
WARNINGSTYLENOL® with Codeine (acetaminophen and codeine phosphate) tablets contain sodium metabisulfite, a sulfite that may cause allergic-type reactions including anaphylactic symptoms and life-threatening or less severe asthmatic episodes in certain susceptible people. The overall prevalence of sulfite sensitivity in the general population is unknown and probably low. Sulfite sensitivity is seen more frequently in asthmatic than in nonasthmatic people.
PRECAUTIONSGeneralHead Injury and Increased Intracranial Pressure: The respiratory depressant effects of narcotics and their capacity to elevate cerebrospinal fluid pressure may be markedly exaggerated in the presence of head injury, other intracranial lesions or a pre-existing increase in intracranial pressure. Furthermore, narcotics produce adverse reactions which may obscure the clinical course of patients with head injuries. Acute Abdominal Conditions: The administration of this product or other narcotics may obscure the diagnosis or clinical course of patients with acute abdominal conditions. Special Risk Patients: This drug should be given with caution to certain patients such as the elderly or debilitated, and those with severe impairment of hepatic or renal function, hypothyroidism, Addison's disease, and prostatic hypertrophy or urethral stricture. Information for PatientsCodeine may impair the mental and/or physical abilities required for the performance of potentially hazardous tasks such as driving a car or operating machinery. The patient using this drug should be cautioned accordingly. The patient should understand the single-dose and 24 hour dose limits, and the time interval between doses. Drug InteractionsPatients receiving other narcotic analgesics, antipsychotics, antianxiety agents, or other CNS depressants (including alcohol) concomitantly with this drug may exhibit an additive CNS depression. When such combined therapy is contemplated, the dose of one or both agents should be reduced. The concurrent use of anticholinergics with codeine may produce paralytic ileus. Carcinogenesis, Mutagenesis, Impairment of FertilityNo long-term studies in animals have been performed with acetaminophen or codeine to determine carcinogenic potential or effects on fertility. Acetaminophen and codeine have been found to have no mutagenic potential using the Ames Salmonella-Microsomal Activation test, the Basc test on Drosophila germ cells, and the Micronucleus test on mouse bone marrow. PregnancyTeratogenic Effects: Pregnancy Category C. Codeine: A study in rats and rabbits reported no teratogenic effect of codeine administered during the period of organogenesis in doses ranging from 5 to 120 mg/kg. In the rat, doses at the 120 mg/kg level, in the toxic range for the adult animal, were associated with an increase in embryo resorption at the time of implantation. In another study a single 100 mg/kg dose of codeine administered to pregnant mice reportedly resulted in delayed ossification in the offspring. There are no studies in humans, and the significance of these findings to humans, if any, is not known. TYLENOL® with Codeine (acetaminophen and codeine phosphate) tablets should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Nonteratogenic Effects: Dependence has been reported in newborns whose mothers took opiates regularly during pregnancy. Withdrawal signs include irritability, excessive crying, tremors, hyperreflexia, fever, vomiting, and diarrhea. These signs usually appear during the first few days of life. Labor and DeliveryNarcotic analgesics cross the placental barrier. The closer to delivery and the larger the dose used, the greater the possibility of respiratory depression in the newborn. Narcotic analgesics should be avoided during labor if delivery of a premature infant is anticipated. If the mother has received narcotic analgesics during labor, newborn infants should be observed closely for signs of respiratory depression. Resuscitation may be required (see OVERDOSAGE ). The effect of codeine, if any, on the later growth, development, and functional maturation of the child is unknown. Nursing MothersSome studies, but not others, have reported detectable amounts of codeine in breast milk. The levels are probably not clinically significant after usual therapeutic dosage. The possibility of clinically important amounts being excreted in breast milk in individuals abusing codeine should be considered. Pediatric UseSafety and effectiveness in pediatric patients have not been established.
ADVERSE REACTIONSThe most frequently observed adverse reactions include lightheadedness, dizziness, sedation, shortness of breath, nausea and vomiting. These effects seem to be more prominent in ambulatory than in non-ambulatory patients, and some of these adverse reactions may be alleviated if the patient lies down. Other adverse reactions include allergic reactions, euphoria, dysphoria, constipation, abdominal pain and pruritus. At higher doses, codeine has most of the disadvantages of morphine including respiratory depression.
DRUG ABUSE AND DEPENDENCETYLENOL® with Codeine (acetaminophen and codeine phosphate) tablets are a Schedule III controlled substance. Codeine can produce drug dependence of the morphine type and, therefore, has the potential for being abused. Psychic dependence, physical dependence and tolerance may develop upon repeated administration of this drug, and it should be prescribed and administered with the same degree of caution appropriate to the use of other oral narcotic-containing medications.
OVERDOSAGEAcetaminophenSigns and Symptoms: In acute acetaminophen overdosage, dose-dependent, potentially fatal hepatic necrosis is the most serious adverse effect. Renal tubular necrosis, hypoglycemic coma and thrombocytopenia may also occur. In adults, hepatic toxicity has rarely been reported with acute overdoses of less than 10 grams and fatalities with less than 15 grams. Importantly, young children seem to be more resistant than adults to the hepatotoxic effect of an acetaminophen overdose. Despite this, the measures outlined below should be initiated in any adult or child suspected of having ingested an acetaminophen overdose. Early symptoms following a potentially hepatotoxic overdose may include: nausea, vomiting, diaphoresis and general malaise. Clinical and laboratory evidence of hepatic toxicity may not be apparent until 48 to 72 hours post-ingestion. Treatment: The stomach should be emptied promptly by lavage or by induction of emesis with syrup of ipecac. Patients' estimates of the quantity of a drug ingested are notoriously unreliable. Therefore, if an acetaminophen overdose is suspected, a serum acetaminophen assay should be obtained as early as possible, but no sooner than four hours following ingestion. Liver function studies should be obtained initially and repeated at 24 hour intervals. The antidote, N-acetylcysteine, should be administered as early as possible, preferably within 16 hours of the overdose ingestion for optimal results, but in any case, within 24 hours. Following recovery, there are no residual, structural or functional hepatic abnormalities. CodeineSigns and Symptoms: Serious overdose with codeine is characterized by respiratory depression (a decrease in respiratory rate and/or tidal volume, Cheyne-Stokes respiration, cyanosis), extreme somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, and sometimes bradycardia and hypotension. In severe overdosage, apnea, circulatory collapse, cardiac arrest and death may occur. Treatment: Primary attention should be given to the reestablishment of adequate respiratory exchange through provision of a patent airway and the institution of assisted or controlled ventilation. The narcotic antagonist naloxone is a specific antidote against respiratory depression which may result from overdosage or unusual sensitivity to narcotics, including codeine. Therefore, an appropriate dose of naloxone hydrochloride (see package insert) should be administered, preferably by the intravenous route, and simultaneously with efforts at respiratory resuscitation. Since the duration of action of codeine may exceed that of the antagonist, the patient should be kept under continued surveillance and repeated doses of the antagonist should be administered as needed to maintain adequate respiration. An antagonist should not be administered in the absence of clinically significant respiratory or cardiovascular depression. Oxygen, intravenous fluids, vasopressors and other supportive measures should be employed as indicated. Gastric emptying may be useful in removing unabsorbed drug.
DOSAGE AND ADMINISTRATIONDosage should be adjusted according to severity of pain and response of the patient. It should be kept in mind, however, that tolerance to codeine can develop with continued use and that the incidence of untoward effects is dose related. Adult doses of codeine higher than 60 mg fail to give commensurate relief of pain but merely prolong analgesia and are associated with an appreciably increased incidence of undesirable side effects. The usual adult dosage for tablets is:
Doses may be repeated up to every 4 hours. The prescriber must determine the number of tablets per dose, and the maximum number of tablets per 24 hours, based upon the above dosage guidance. This information should be conveyed in the prescription.
HOW SUPPLIEDTYLENOL® with Codeine (acetaminophen and codeine phosphate) tablets: are white, round, flat-faced, beveled edged tablets imprinted "McNEIL," on one side and "TYLENOL CODEINE" and either "3" or "4" on the other side and are supplied as follows: No. 3 - NDC 0045-0513-60 bottles of 100, NDC 0045-0513-80 bottles of 1000, No. 4 - NDC 0045-0515-60 bottles of 100, NDC 0045-0515-70 bottles of 500. Store TYLENOL with Codeine tablets at controlled room temperature 15°-30°C (59°-86°F). Dispense in tight, light-resistant container as defined in the official compendium. OMP DIVISION Ortho-Mcneil PHARMACEUTICAL, INC. Raritan, New Jersey 08869 © OMP 2000 Revised October 2004 7518402
|
 - To bookmark this page (add it to your favorites), please click the image to the left.
- To bookmark this page (add it to your favorites), please click the image to the left.